

Preliminary study of buprenorphine and bupropion for opioid-dependent smokers
- PMID: 18612883
- PMCID: PMC2588345
- DOI: 10.1080/10550490802138814
Preliminary study of buprenorphine and bupropion for opioid-dependent smokers
Abstract
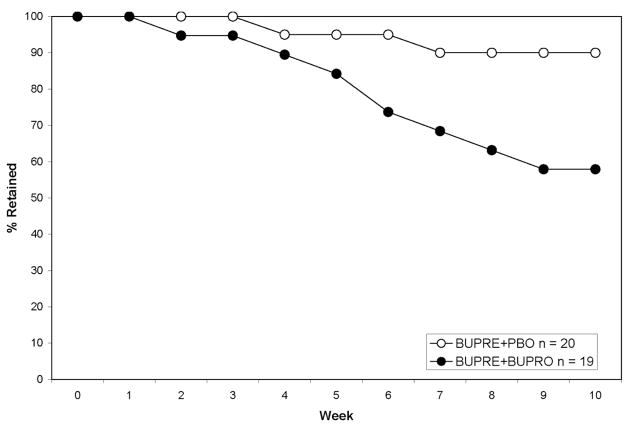
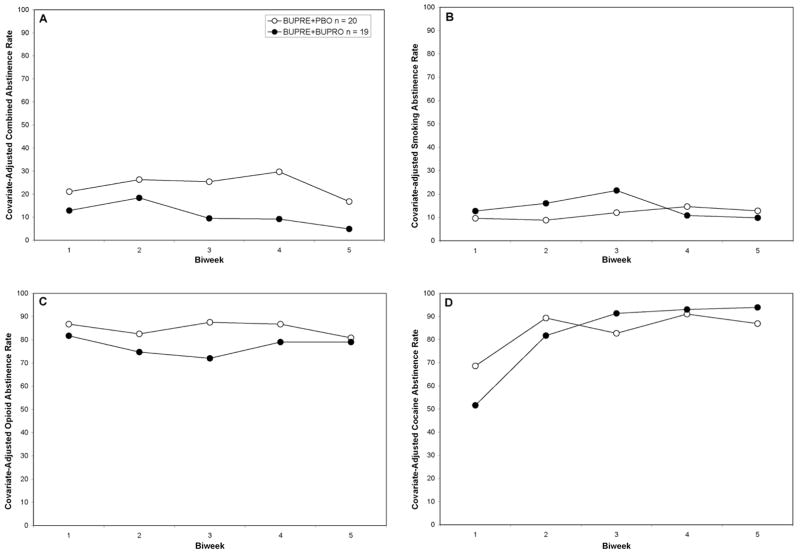
In this double-blind, placebo-controlled trial, bupropion (BUPRO, 300 mg/day) was compared to placebo (PBO) for the concurrent treatment of opioid and tobacco addiction in 40 opioid-dependent smokers stabilized on buprenorphine (BUPRE, 24 mg/day). Participants received contingent, monetary reinforcement for abstinence from smoking, illicit opioids, and cocaine. Significant differences in treatment retention were observed (BUPRE+BUPRO, 58%; BUPRE+PBO, 90%). BUPRO treatment was not more effective than placebo for abstinence from tobacco, opioids, or cocaine in BUPRE-stabilized patients. These preliminary findings do not support the efficacy of BUPRO, in combination with BUPRE, for the concurrent treatment of opioid and tobacco addiction.
Figures
References
-
- McCool RM, Richter KP, Choi WS. Benefits of and barriers to providing smoking treatment in methadone clinics: findings from a national study. Am J Addict. 2005;14(4):358–366. - PubMed
-
- Pomerleau OF. Endogenous opioids and smoking: a review of progress and problems. Psychoneuroendocrinology. 1998;23(2):115–130. - PubMed
-
- Mello NK, Lukas SE, Mendelson JH. Buprenorphine effects on cigarette smoking. Psychopharmacology (Berl) 1985;86(4):417–425. - PubMed
-
- Mello NK, Mendelson JH, Sellers ML, Kuehnle JC. Effects of heroin self-administration on cigarette smoking. Psychopharmacology (Berl) 1980;67(1):45–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
