

Public-health and individual approaches to antiretroviral therapy: township South Africa and Switzerland compared
- PMID: 18613745
- PMCID: PMC2443185
- DOI: 10.1371/journal.pmed.0050148
Public-health and individual approaches to antiretroviral therapy: township South Africa and Switzerland compared
Erratum in
- PLoS Med. 2008 Sep;5(9):e195
Abstract
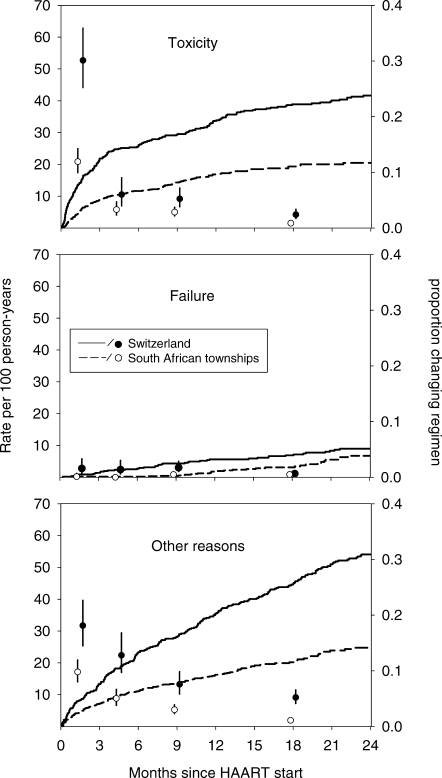
Background: The provision of highly active antiretroviral therapy (HAART) in resource-limited settings follows a public health approach, which is characterised by a limited number of regimens and the standardisation of clinical and laboratory monitoring. In industrialized countries doctors prescribe from the full range of available antiretroviral drugs, supported by resistance testing and frequent laboratory monitoring. We compared virologic response, changes to first-line regimens, and mortality in HIV-infected patients starting HAART in South Africa and Switzerland.
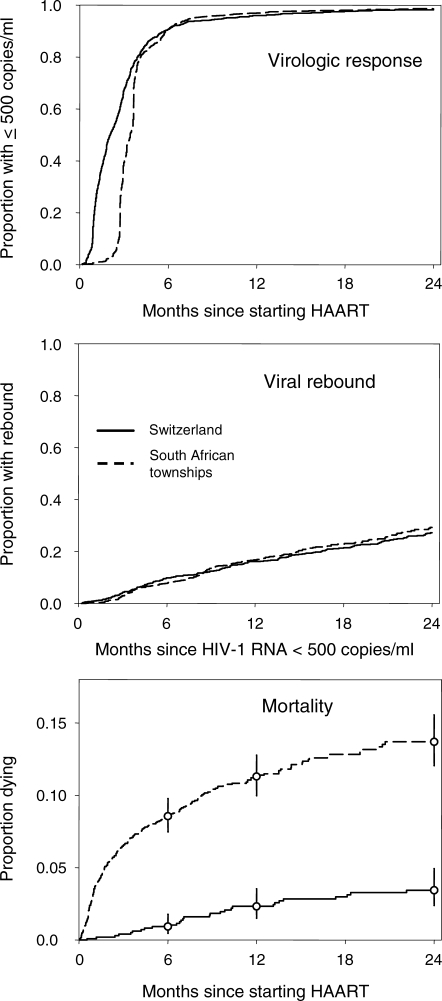
Methods and findings: We analysed data from the Swiss HIV Cohort Study and two HAART programmes in townships of Cape Town, South Africa. We included treatment-naïve patients aged 16 y or older who had started treatment with at least three drugs since 2001, and excluded intravenous drug users. Data from a total of 2,348 patients from South Africa and 1,016 patients from the Swiss HIV Cohort Study were analysed. Median baseline CD4+ T cell counts were 80 cells/mul in South Africa and 204 cells/mul in Switzerland. In South Africa, patients started with one of four first-line regimens, which was subsequently changed in 514 patients (22%). In Switzerland, 36 first-line regimens were used initially, and these were changed in 539 patients (53%). In most patients HIV-1 RNA was suppressed to 500 copies/ml or less within one year: 96% (95% confidence interval [CI] 95%-97%) in South Africa and 96% (94%-97%) in Switzerland, and 26% (22%-29%) and 27% (24%-31%), respectively, developed viral rebound within two years. Mortality was higher in South Africa than in Switzerland during the first months of HAART: adjusted hazard ratios were 5.90 (95% CI 1.81-19.2) during months 1-3 and 1.77 (0.90-3.50) during months 4-24.
Conclusions: Compared to the highly individualised approach in Switzerland, programmatic HAART in South Africa resulted in similar virologic outcomes, with relatively few changes to initial regimens. Further innovation and resources are required in South Africa to both achieve more timely access to HAART and improve the prognosis of patients who start HAART with advanced disease.
Conflict of interest statement
Figures
References
-
- World Health Organization. Recommendations for a public health approach. Geneva: WHO; 2006. Antiretroviral therapy for HIV Infection in adults and adolescents in resource-limited settings: towards universal access. Available at: http://www.who.int/hiv/pub/guidelines/WHO%20Adult%20ART%20Guidelines.pdf. Accessed 5 June 2008.
-
- Gilks CF, Crowley S, Ekpini R, Gove S, Perriens J, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–510. - PubMed
-
- Beck EJ, Vitoria M, Mandalia S, Crowley S, Gilks CF, et al. National adult antiretroviral therapy guidelines in resource-limited countries: concordance with 2003 WHO guidelines. AIDS. 2006;20:1497–1502. - PubMed
-
- World Health Organisation, UNAIDS, UNICEF. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress Report, April 2007. Geneva: WHO; 2007. Available at: http://libdoc.who.int/publications/2007/9789241595391_eng.pdf. Accessed 5 June 2008.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
