

Staged surgical treatment for severe and rigid scoliosis
- PMID: 18613982
- PMCID: PMC2481248
- DOI: 10.1186/1749-799X-3-26
Staged surgical treatment for severe and rigid scoliosis
Abstract
Background: A retrospective study of staged surgery for severe rigid scoliosis. The purpose of this study was to evaluate the result of staged surgery in treatment of severe rigid scoliosis and to discuss the indications.
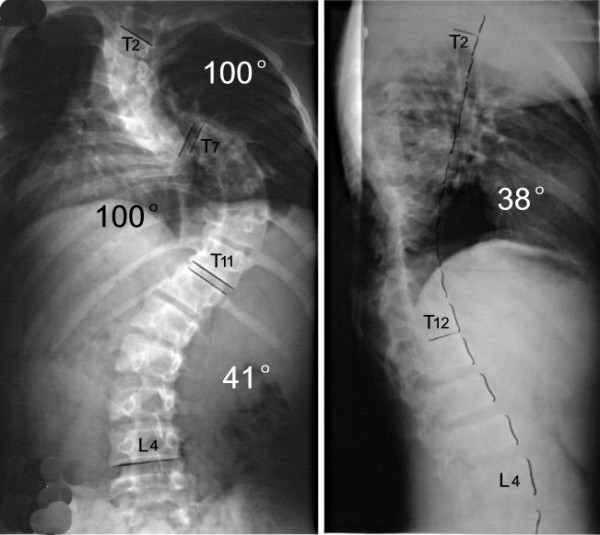
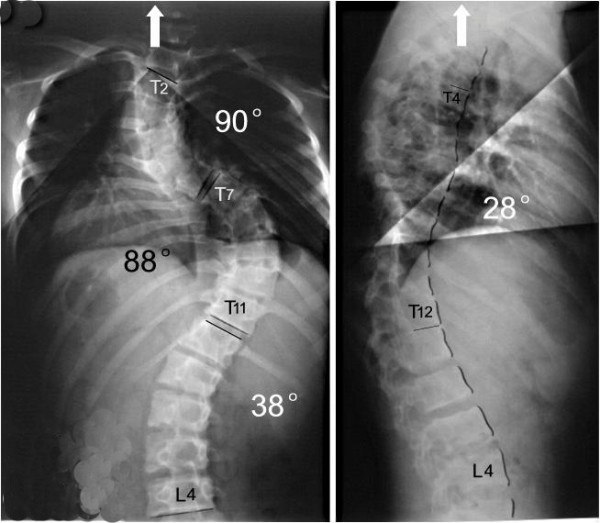
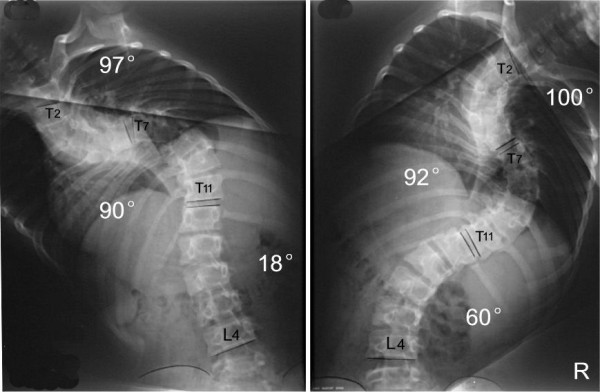
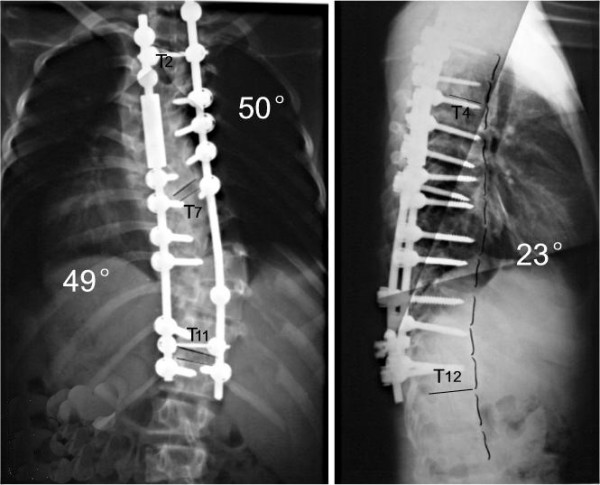
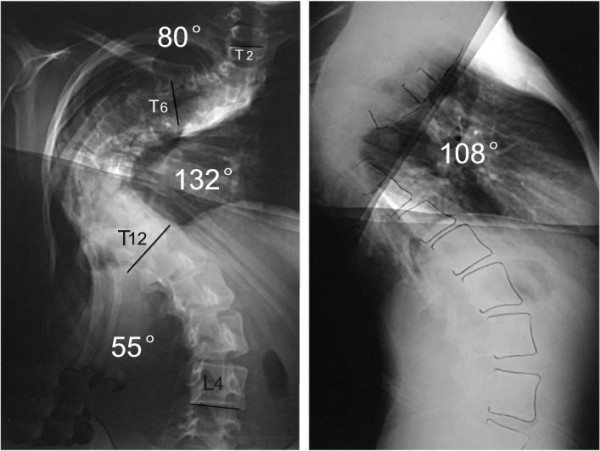
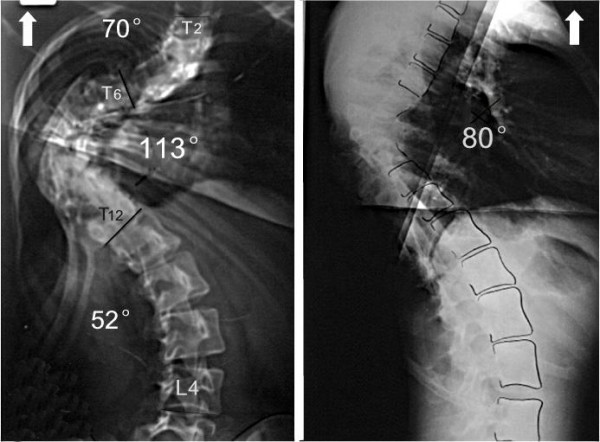
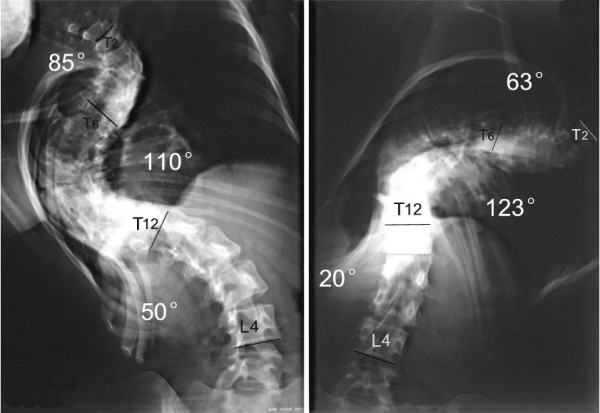
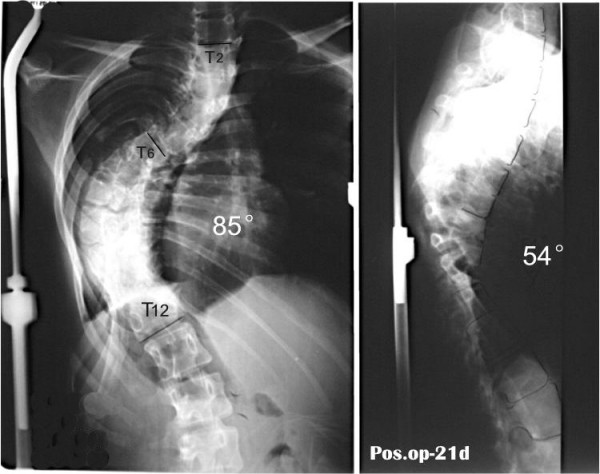
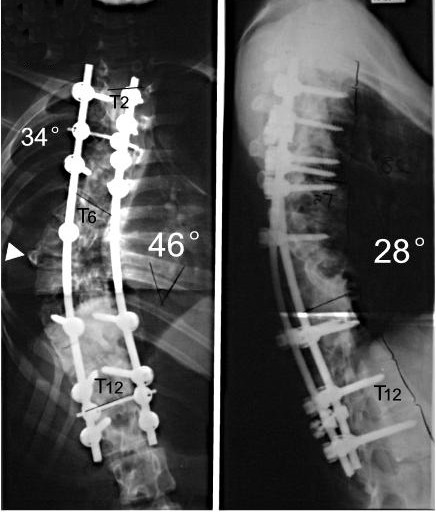
Methods: From 1998 to 2006, 21 cases of severe rigid scoliosis with coronal Cobb angle more than 80 degrees were treated by staged surgeries including anterior release and halo-pelvic traction as first stage surgery and posterior instrumentation and spinal fusion as second stage. Pedicle subtraction osteotomy(PSO) was added in second stage according to spine rigidity. Among the 21 patients, 8 were male and 13 female with an average age of 15.3 years (rang from 4 to 23 years). The mean pre-operative Cobb angle was 110.5 degrees (80 degrees -145 degrees ) with a mean spine flexibility of 13%. Radiological parameters at different operative time points were analyzed (mean time of follow-up: 51 months).
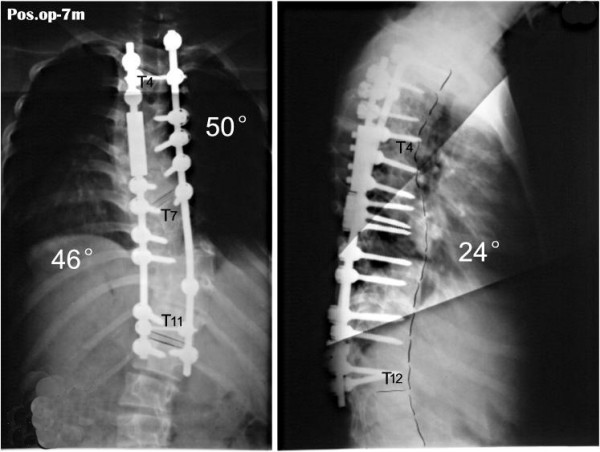
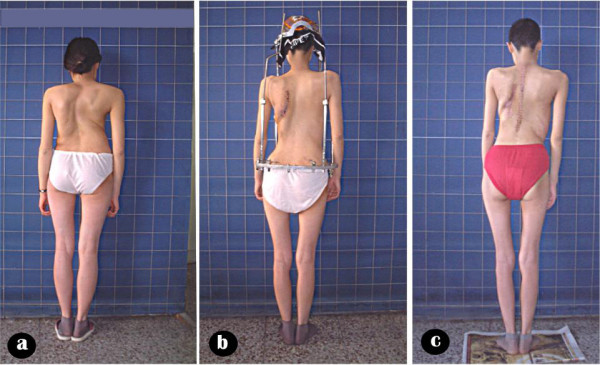
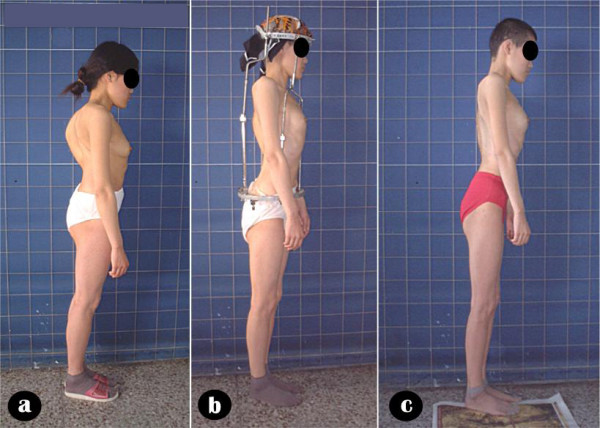
Results: External appearance of all patients improved significantly. The average correction rate was 65.2% (ranging from 39.8% to 79.5%) with mean correction loss of 2.23 degrees at the end of follow-up. No decompensation of trunk has been found. Mean distance between the midline of C7 and midsacral line was 1.19 cm +/- 0.51. Two patients had neurological complications: one patient had motor deficit and recovered incompletely.
Conclusion: Staged operation and halo-pelvic traction offer a safe and effective way in treatment of severe rigid scoliosis. Patients whose Cobb angle was more than 80 degrees and the flexibility of the spine was less than 20% should be treated in this way, and those whose flexibility of the spine was less than 10% and the Cobb angle remained more than 70 degrees after 1st stage anterior release and halo-pelvic traction should undergo pedicle subtraction osteotomy (PSO) in the second surgery.
Figures



References
-
- Luque ER. The correction of postural curves of Spine. 1982. p. 270. - PubMed
-
- Dutoit M, Rigault P, Pouliquen JC, Padovani JP, Beneux J, Pasteyer J, Merckx J, Guyonvarch G. Surgical treatment of scoliosis of 100 degrees and greater in children and adolescent (neurological and myopathic scoliosis excluded). Apropos of a series of 66 cases. Rev Chir orthop Reparatrice Appar Mot. 1985;71:549–562. - PubMed
-
- Shi YM, Hou SX, Li L, Wang HD, Gao TJ, Wei X. Prevention and management of the neurological complications during the treatment of severe scoliosis. Zhonghua Wai Ke Za Zhi. 45:517–9. 2007 Apr 15. - PubMed
-
- Zhang YG, Wang Y, Zhang XS. [Clinical study on transpedicular spinal osteotomy and vertebrectomy in 125 cases of severe rigid spinal deformity] Zhonghua Wai Ke Za Zhi. 45:525–8. 2007 Apr 15. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
