

Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample
- PMID: 18613993
- PMCID: PMC3536475
- DOI: 10.4065/83.7.765
Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample
Abstract
Objective: To describe the spectrum of visits to US emergency departments (EDs) for acute dizziness and determine whether ED patients with dizziness are diagnosed as having a range of benign and dangerous medical disorders, rather than predominantly vestibular ones.
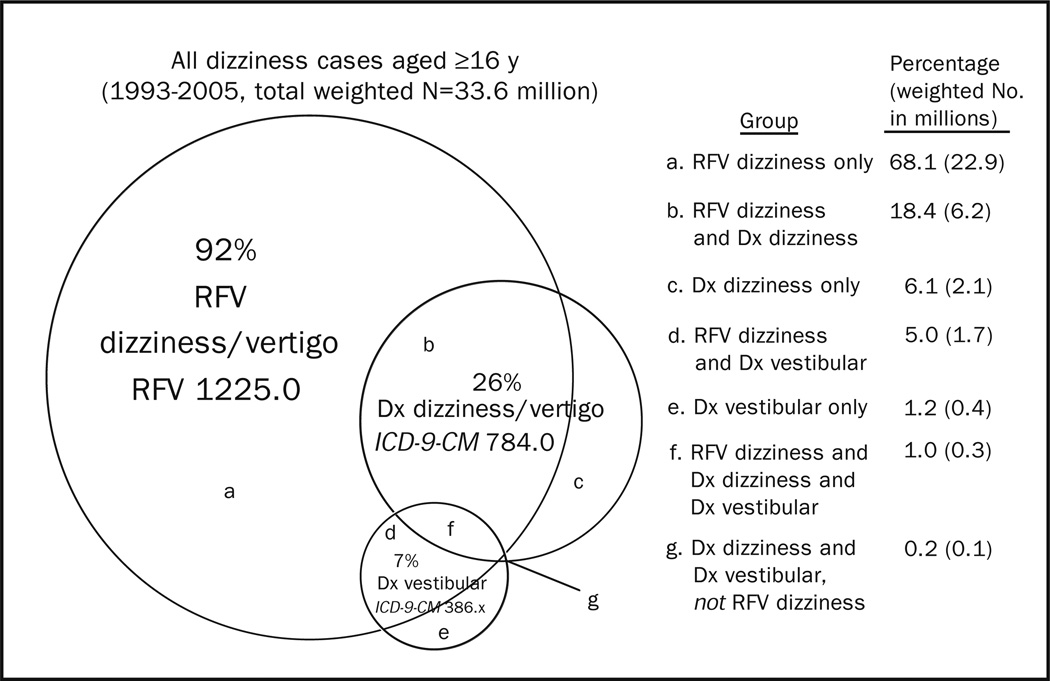
Patients and methods: A cross-sectional study of ED visits from the National Hospital Ambulatory Medical Care Survey (NHAMCS) used a weighted sample of US ED visits (1993-2005) to measure patient and hospital demographics, ED diagnoses, and resource use in cases vs controls without dizziness. Dizziness in patients 16 years or older was defined as an NHAMCS reason-for-visit code of dizziness/vertigo (1225.0) or a final International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis of dizziness/vertigo (780.4) or of a vestibular disorder (386.x).
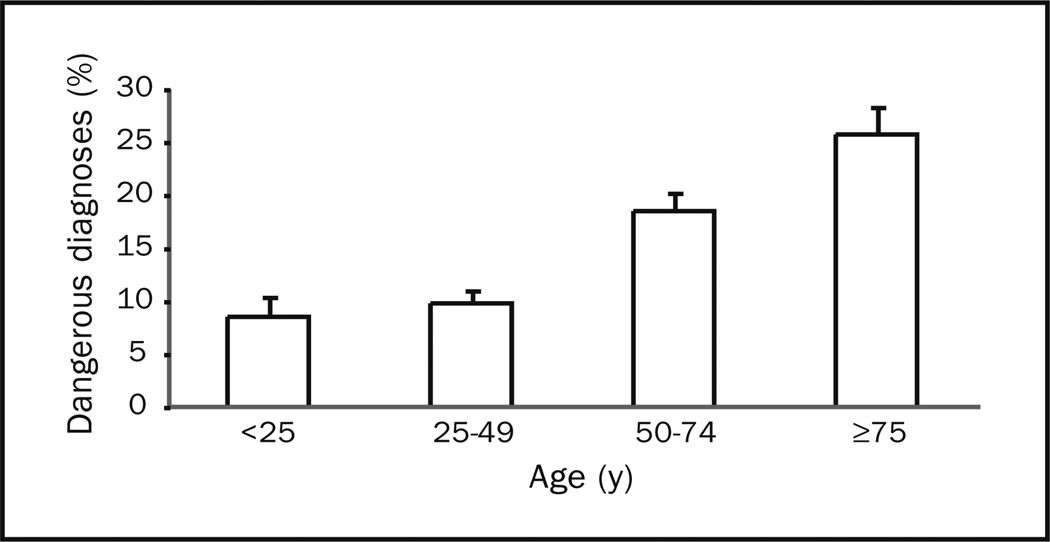
Results: A total of 9472 dizziness cases (3.3% of visits) were sampled over 13 years (weighted 33.6 million). Top diagnostic groups were otologic/vestibular (32.9%), cardiovascular (21.1%), respiratory (11.5%), neurologic (11.2%, including 4% cerebrovascular), metabolic (11.0%), injury/poisoning (10.6%), psychiatric (7.2%), digestive (7.0%), genitourinary (5.1%), and infectious (2.9%). Nearly half of the cases (49.2%) were given a medical diagnosis, and 22.1% were given only a symptom diagnosis. Predefined dangerous disorders were diagnosed in 15%, especially among those older than 50 years (20.9% vs 9.3%; P<.001). Dizziness cases were evaluated longer (mean 4.0 vs 3.4 hours), imaged disproportionately (18.0% vs 6.9% undergoing computed tomography or magnetic resonance imaging), and admitted more often (18.8% vs 14.8%) (all P<.001).
Conclusion: Dizziness is not attributed to a vestibular disorder in most ED cases and often is associated with cardiovascular or other medical causes, including dangerous ones. Resource use is substantial, yet many patients remain undiagnosed.
Figures
Comment in
-
Diagnosing dizziness in the emergency and primary care settings.Mayo Clin Proc. 2008 Nov;83(11):1297-8; author reply 1298-9. doi: 10.4065/83.11.1297-a. Mayo Clin Proc. 2008. PMID: 18990331 No abstract available.
References
-
- Kroenke K, Jackson JL. Outcome in general medical patients presenting with common symptoms: a prospective study with a 2-week and a 3-month follow-up. Fam Pract. 1998;15(5):398–403. - PubMed
-
- Newman-Toker DE, Cannon LM, Stofferahn ME, Rothman RE, Hsieh YH, Zee DS. Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting. Mayo Clin Proc. 2007;82(11):1329–1340. - PubMed
-
- Herr RD, Zun L, Mathews JJ. A directed approach to the dizzy patient. Ann Emerg Med. 1989;18(6):664–672. - PubMed
-
- Skiendzielewski JJ, Martyak G. The weak and dizzy patient. Ann Emerg Med. 1980;9(7):353–356. - PubMed
-
- Kroenke K, Hoffman RM, Einstadter D. How common are various causes of dizziness? a critical review. South Med J. 2000;93(2):160–167. - PubMed
