

Androgen receptor-negative human prostate cancer cells induce osteogenesis in mice through FGF9-mediated mechanisms
- PMID: 18618013
- PMCID: PMC2447924
- DOI: 10.1172/JCI33093
Androgen receptor-negative human prostate cancer cells induce osteogenesis in mice through FGF9-mediated mechanisms
Abstract
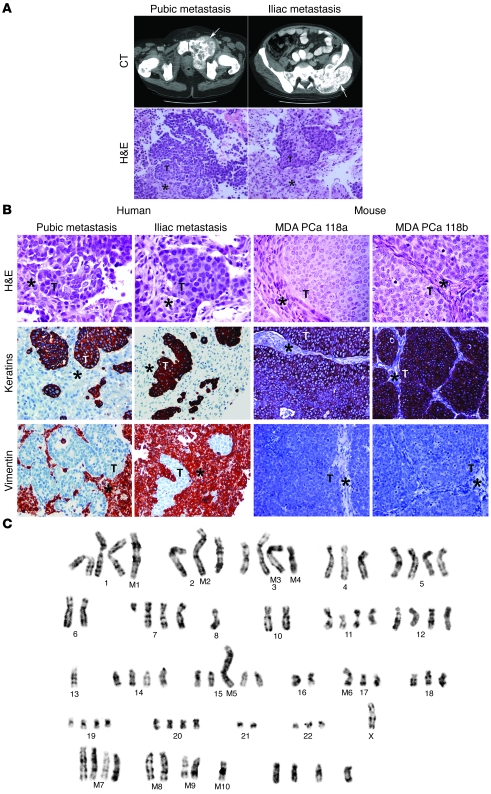
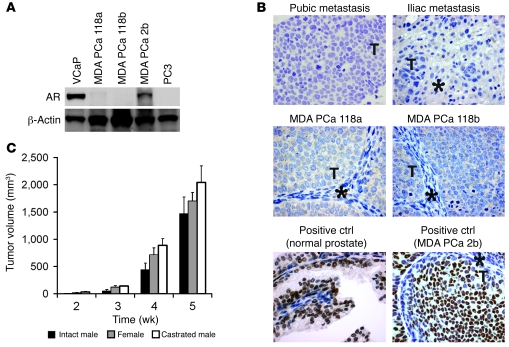
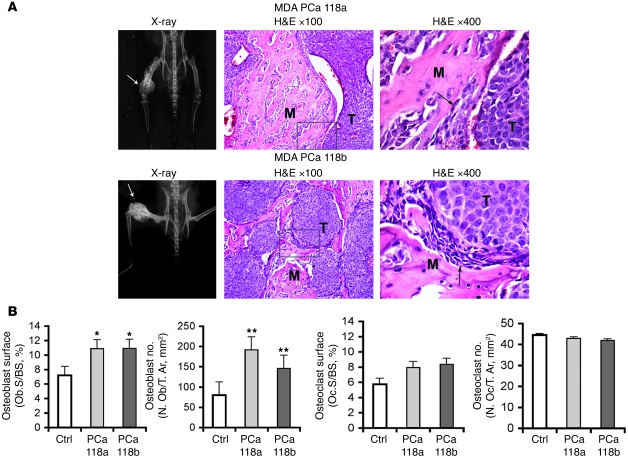
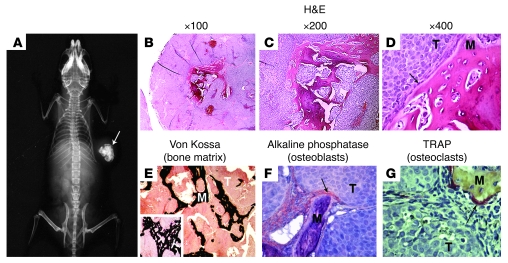
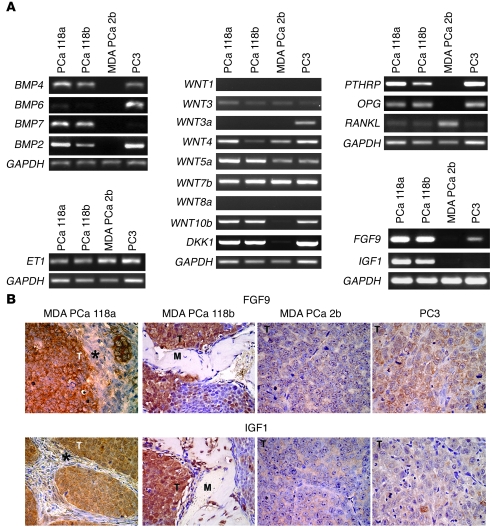
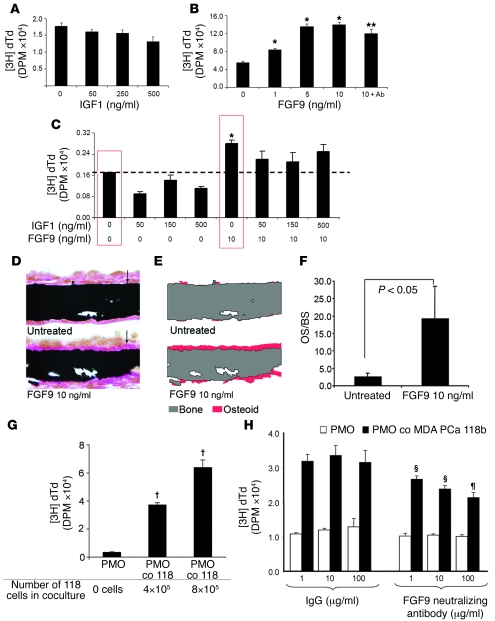
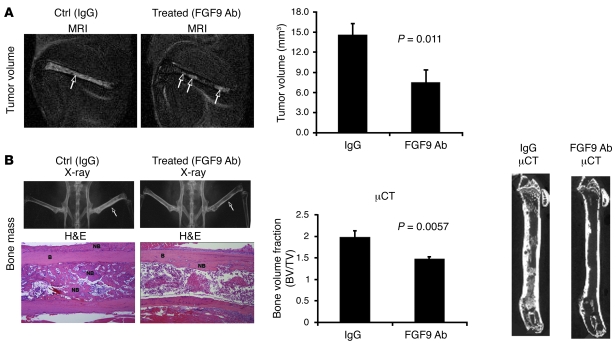
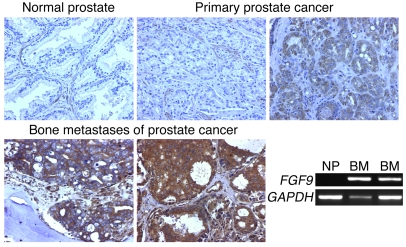
In prostate cancer, androgen blockade strategies are commonly used to treat osteoblastic bone metastases. However, responses to these therapies are typically brief, and the mechanism underlying androgen-independent progression is not clear. Here, we established what we believe to be the first human androgen receptor-negative prostate cancer xenografts whose cells induced an osteoblastic reaction in bone and in the subcutis of immunodeficient mice. Accordingly, these cells grew in castrated as well as intact male mice. We identified FGF9 as being overexpressed in the xenografts relative to other bone-derived prostate cancer cells and discovered that FGF9 induced osteoblast proliferation and new bone formation in a bone organ assay. Mice treated with FGF9-neutralizing antibody developed smaller bone tumors and reduced bone formation. Finally, we found positive FGF9 immunostaining in prostate cancer cells in 24 of 56 primary tumors derived from human organ-confined prostate cancer and in 25 of 25 bone metastasis cases studied. Collectively, these results suggest that FGF9 contributes to prostate cancer-induced new bone formation and may participate in the osteoblastic progression of prostate cancer in bone. Androgen receptor-null cells may contribute to the castration-resistant osteoblastic progression of prostate cancer cells in bone and provide a preclinical model for studying therapies that target these cells.
Figures

References
-
- Jemal A., et al. Cancer statistics, 2007. CA Cancer J. Clin. 2007;57:43–66. - PubMed
-
- Cook G.B., Watson F.R. Events in the natural history of prostate cancer: using salvage curves, mean age distributions and contingency coefficients. J. Urol. 1968;99:87–96. - PubMed
-
- Clarke N.W., McClure J., George N.I. Osteoblast function and osteomalacia in metastatic prostate cancer. Eur. Urol. 1993;24:286–290. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
