

Integration of depression and hypertension treatment: a pilot, randomized controlled trial
- PMID: 18626028
- PMCID: PMC2478504
- DOI: 10.1370/afm.843
Integration of depression and hypertension treatment: a pilot, randomized controlled trial
Abstract
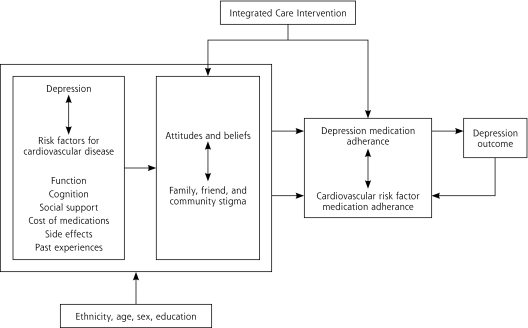
Purpose: We wanted to examine whether integrating depression treatment into care for hypertension improved adherence to antidepressant and antihypertensive medications, depression outcomes, and blood pressure control among older primary care patients.
Methods: Older adults prescribed pharmacotherapy for depression and hypertension from physicians at a large primary care practice in West Philadelphia were randomly assigned to an integrated care intervention or usual care. Outcomes were assessed at baseline, 2, 4, and 6 weeks using the Center for Epidemiologic Studies Depression Scale (CES-D) to assess depression, an electronic monitor to measure blood pressure, and the Medication Event Monitoring System to assess adherence.
Results: In all, 64 participants aged 50 to 80 years participated. Participants in the integrated care intervention had fewer depressive symptoms (CES-D mean scores, intervention 9.9 vs usual care 19.3; P <.01), lower systolic blood pressure (intervention 127.3 mm Hg vs usual care 141.3 mm Hg; P <.01), and lower diastolic blood pressure (intervention 75.8 mm Hg vs usual care 85.0 mm Hg; P <.01) compared with participants in the usual care group at 6 weeks. Compared with the usual care group, the proportion of participants in the intervention group who had 80% or greater adherence to an antidepressant medication (intervention 71.9% vs usual care 31.3%; P <.01) and to an antihypertensive medication (intervention 78.1% vs usual care 31.3%; P <.001) was greater at 6 weeks.
Conclusion: A pilot, randomized controlled trial integrating depression and hypertension treatment was successful in improving patient outcomes. Integrated interventions may be more feasible and effective in real-world practices, where there are competing demands for limited resources.
Figures
References
-
- Rabins PV. Prevention of mental disorders in the elderly: current perspectives and future prospects. J Am Geriatr Soc. 1992;40(7): 727–733. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical