

Classification of traumatic brain injury for targeted therapies
- PMID: 18627252
- PMCID: PMC2721779
- DOI: 10.1089/neu.2008.0586
Classification of traumatic brain injury for targeted therapies
Abstract
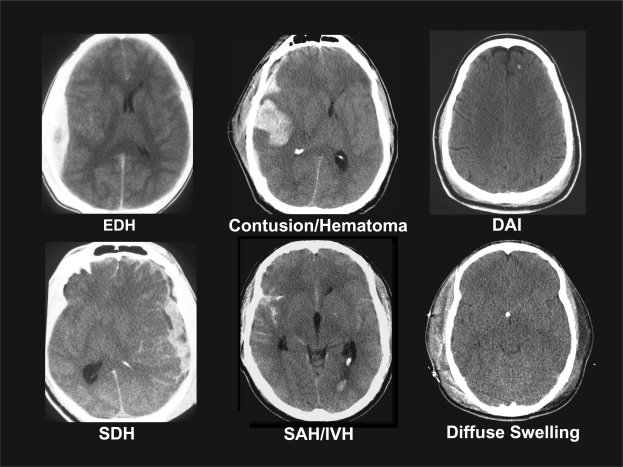
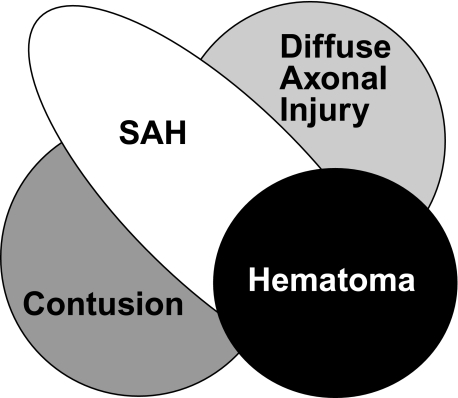
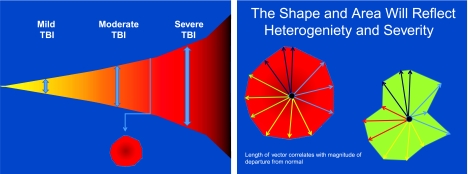
The heterogeneity of traumatic brain injury (TBI) is considered one of the most significant barriers to finding effective therapeutic interventions. In October, 2007, the National Institute of Neurological Disorders and Stroke, with support from the Brain Injury Association of America, the Defense and Veterans Brain Injury Center, and the National Institute of Disability and Rehabilitation Research, convened a workshop to outline the steps needed to develop a reliable, efficient and valid classification system for TBI that could be used to link specific patterns of brain and neurovascular injury with appropriate therapeutic interventions. Currently, the Glasgow Coma Scale (GCS) is the primary selection criterion for inclusion in most TBI clinical trials. While the GCS is extremely useful in the clinical management and prognosis of TBI, it does not provide specific information about the pathophysiologic mechanisms which are responsible for neurological deficits and targeted by interventions. On the premise that brain injuries with similar pathoanatomic features are likely to share common pathophysiologic mechanisms, participants proposed that a new, multidimensional classification system should be developed for TBI clinical trials. It was agreed that preclinical models were vital in establishing pathophysiologic mechanisms relevant to specific pathoanatomic types of TBI and verifying that a given therapeutic approach improves outcome in these targeted TBI types. In a clinical trial, patients with the targeted pathoanatomic injury type would be selected using an initial diagnostic entry criterion, including their severity of injury. Coexisting brain injury types would be identified and multivariate prognostic modeling used for refinement of inclusion/exclusion criteria and patient stratification. Outcome assessment would utilize endpoints relevant to the targeted injury type. Advantages and disadvantages of currently available diagnostic, monitoring, and assessment tools were discussed. Recommendations were made for enhancing the utility of available or emerging tools in order to facilitate implementation of a pathoanatomic classification approach for clinical trials.
Figures
References
-
- Adams J.H. Graham D.I. An Introduction to Neuropathology. Churchill Livingstone: Edinburgh; 1994.
-
- Adams J.H. Graham D.I. Murray L.S. Scott G. Diffuse axonal injury due to nonmissile head injury in humans: an analysis of 45 cases. Ann. Neurol. 1982;12:557–563. - PubMed
-
- Adams J.H. Mitchell D.E. Graham D.I. Doyle D. Diffuse brain damage of immediate impact type. Its relationship to “primary brain-stem damage” in head injury. Brain. 1977;100:489–502. - PubMed
-
- Alderman N. Burgess P.W. Knight C. Henman C. Ecological validity of a simplified version of the multiple errands shopping test. J. Int. Neuropsychol. Soc. 2003;9:31–44. - PubMed
-
- Armonda R.A. Bell R.S. Vo A.H. Ling G. DeGraba T.J. Crandall B. Ecklund J. Campbell W.W. Wartime traumatic cerebral vasospasm: recent review of combat casualties. Neurosurgery. 2006;59:1215–1225. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
