

Glucose intolerance in pregnancy and future risk of pre-diabetes or diabetes
- PMID: 18628572
- PMCID: PMC2551649
- DOI: 10.2337/dc08-0972
Glucose intolerance in pregnancy and future risk of pre-diabetes or diabetes
Abstract
Objective: The purpose of this study was to test the hypothesis that any degree of abnormal glucose homeostasis detected on antepartum screening for gestational diabetes mellitus (GDM) should be associated with an increased risk of postpartum pre-diabetes or diabetes.
Research design and methods: In this prospective cohort study, 487 women underwent 1) antepartum GDM screening by a glucose challenge test (GCT) and a diagnostic oral glucose tolerance test (OGTT) and 2) postpartum metabolic characterization by OGTT at 3 months after delivery. Four baseline glucose tolerance groups were defined on the basis of the antepartum GCT/OGTT: 1) GDM (n = 137); 2) gestational impaired glucose tolerance (GIGT) (n = 91); 3) abnormal GCT with normal glucose tolerance on an OGTT (abnormal GCT NGT) (n = 166); and 4) normal GCT with NGT on an OGTT (normal GCT NGT) (n = 93).
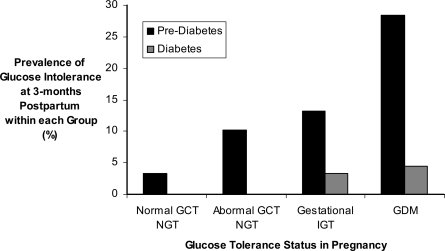
Results: The prevalence of postpartum glucose intolerance (pre-diabetes or diabetes) increased across the groups from normal GCT NGT (3.2%) to abnormal GCT NGT (10.2%) to GIGT (16.5%) to GDM (32.8%) (P(trend) < 0.0001). On logistic regression analysis, all three categories of abnormal glucose homeostasis in pregnancy independently predicted postpartum glucose intolerance: abnormal GCT NGT odds ratio (OR) 3.6 (95% CI 1.01-12.9); GIGT OR 5.7 (1.6-21.1); and GDM OR 14.3 (4.2-49.1). Furthermore, both in pregnancy and at 3 months postpartum, insulin sensitivity (IS(OGTT)) and pancreatic beta-cell function (insulinogenic index/homeostasis model assessment of insulin resistance) progressively decreased across the groups from normal GCT NGT to abnormal GCT NGT to GIGT to GDM (all P(trend) < 0.0001).
Conclusions: Any degree of abnormal glucose homeostasis in pregnancy independently predicts an increased risk of glucose intolerance postpartum.
Figures
References
-
- Kim C, Newton KM, Knopp RH: Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 25:1862–1868, 2002 - PubMed
-
- Kahn SE: The relative contributions of insulin resistance and β-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia 46:3–19, 2003 - PubMed
-
- Buchanan TA: Pancreatic β-cell defects in gestational diabetes: implications for the pathogenesis and prevention of type 2 diabetes. J Clin Endocrinol Metab 86:989–993, 2001 - PubMed
-
- Hanna FW, Peters JR: Screening for gestational diabetes. Diabet Med 19:351–358, 2002 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
