

Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formation
- PMID: 18628972
- PMCID: PMC2446413
- DOI: 10.1080/08998280.2008.11928404
Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formation
Abstract
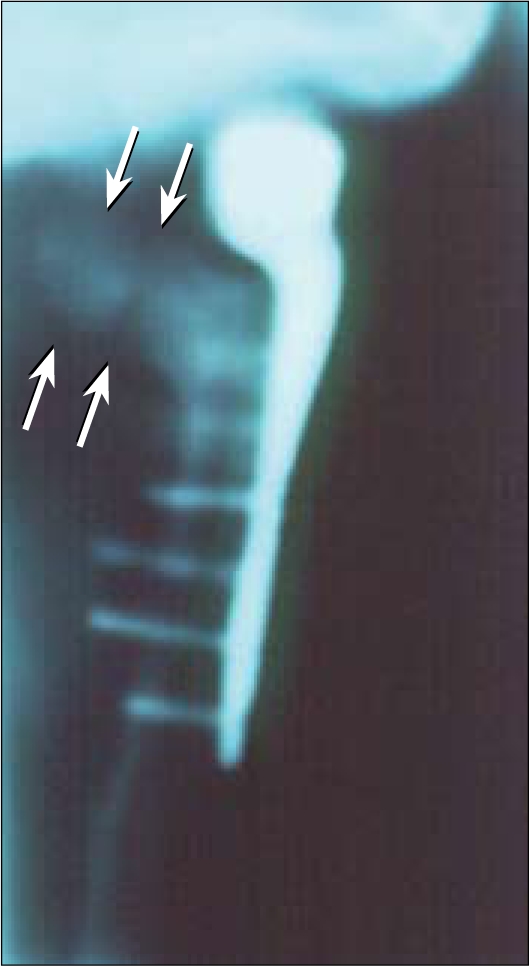
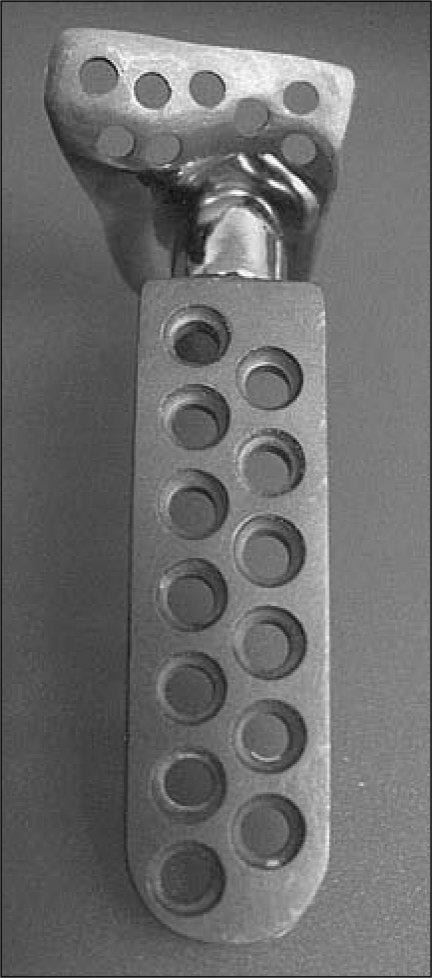
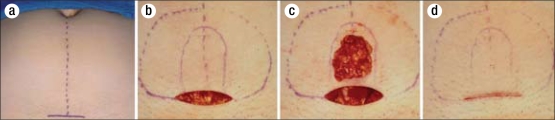
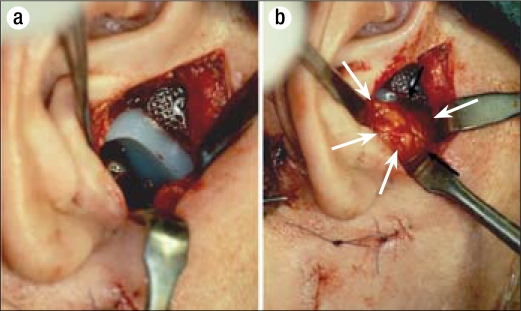
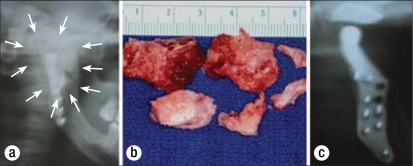
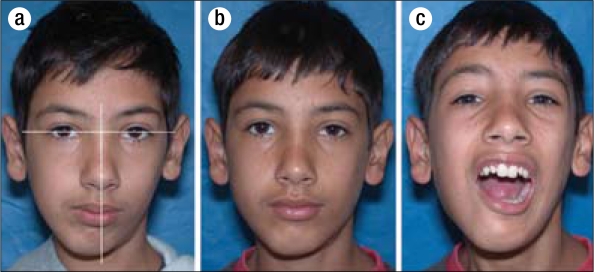
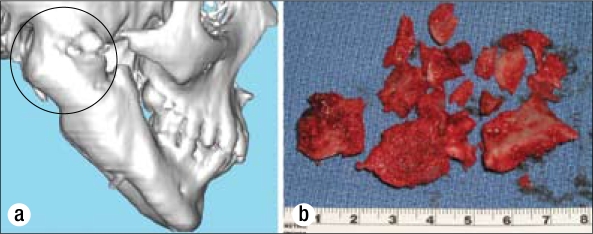
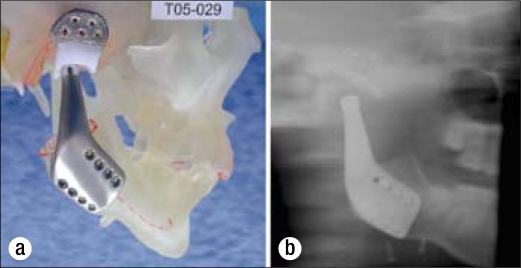
This study evaluated 1) the efficacy of packing autologous fat grafts around temporomandibular joint (TMJ) total joint prosthetic reconstructions to prevent fibrosis and heterotopic bone formation and 2) the effects on postsurgical joint mobility and jaw function. One hundred fifteen patients (5 males and 110 females) underwent TMJ reconstruction with total joint prostheses and simultaneous fat grafts (88 bilateral and 27 unilateral) for a total of 203 joints. The abdominal fat grafts were packed around the articulating portion of the joint prostheses after the fossa and mandibular components were stabilized. Patients were divided into two groups: group 1 (n = 76 joints) received Christensen total joint prostheses, and group 2 (n = 127 joints) received TMJ Concepts total joint prostheses. Clinical and radiographic assessments were performed before surgery, immediately after surgery, and at long-term follow-up. In group 1, maximal incisal opening (MIO) increased 3.5 mm, lateral excursions (LE) decreased 0.2 mm, and jaw function improved 1.9 levels. In group 2, MIO increased 6.8 mm, LE decreased 1.4 mm, and jaw function improved 2.4 levels. The improvement for MIO and patient perception of jaw function in both groups was statistically significant; no significant difference was found for LE. There was no radiographic or clinical evidence of heterotopic calcifications or limitation of mobility secondary to fibrosis in either group. Twenty-five Christensen prostheses (33%) were removed because of device failure and/or metal hypersensitivity; no fibrosis or heterotopic bone formation was seen at surgical removal. Four TMJ Concepts prostheses (3%) were removed because of metal hypersensitivity. In all instances, removal of the prostheses was unrelated to the autologous fat grafting. Ten patients (8.7%) developed complications involving the fat donor site: two patients (1.8%) developed abdominal cysts requiring surgery, and eight patients (6.9%) developed seroma formation requiring aspiration. Autologous fat transplantation is a useful adjunct to prosthetic TMJ reconstruction to minimize the occurrence of excessive joint fibrosis and heterotopic calcification, consequently providing improved range of motion and jaw function.
Figures



References
-
- Neuber H. Fettransplantation. Chir Kong Verhandl. 1893;1:66.
-
- Blair VP. Operative treatment of ankylosis of the mandible. Trans South Surg Assoc. 1913;28:435.
-
- Murphy JB. Arthroplasty for intra-articular bony and fibrous ankylosis of the temporomandibular articulation. JAMA. 1914;62:1783.
-
- Tomas BJ. Heterotopic bone formation after total hip arthroplasty. Orthop Clin North Am. 1992;23(2):347–358. - PubMed
-
- Fingeroth RJ, Ahmed AQ. Single dose 6 Gy prophylaxis for heterotopic ossification after total hip arthroplasty. Clin Orthop Relat Res. 1995;317:131–140. - PubMed
LinkOut - more resources
Full Text Sources