

The impact of automated eGFR reporting and education on nephrology service referrals
- PMID: 18632591
- PMCID: PMC2639066
- DOI: 10.1093/ndt/gfn385
The impact of automated eGFR reporting and education on nephrology service referrals
Abstract
Background: Serum creatinine concentration is an unreliable and insensitive marker of chronic kidney disease (CKD). To improve CKD detection, the Australasian Creatinine Consensus Working Committee recommended reporting of estimated glomerular filtration rate (eGFR) using the four-variable Modification of Diet in Renal Disease (MDRD) formula with every request for serum creatinine concentration. The aim of this study was to evaluate the impact of automated laboratory reporting of eGFR on the quantity and quality of referrals to nephrology services in Southeast Queensland, Australia.
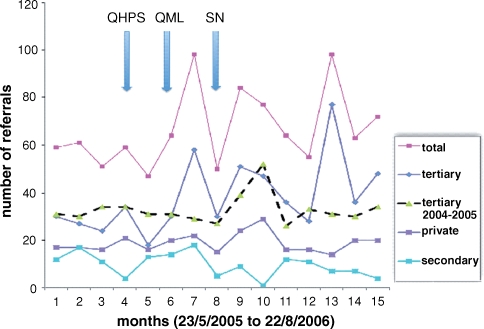
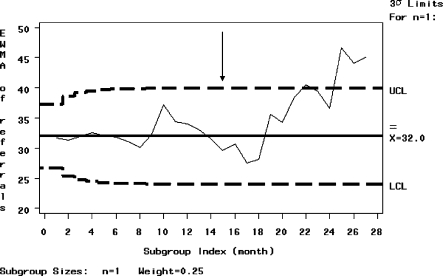
Methods: Outpatient referrals to a tertiary and regional renal service, and a single private practice were prospectively audited over 3-12 months prior to and 12 months following the introduction of automated eGFR reporting and concomitant clinician education. The appropriateness of referrals to a nephrologist was assessed according to the Kidney Check Australia Taskforce (KCAT) criteria. Significant changes in the quantity and/or quality of referrals over time were analysed by exponentially weighed moving average (EWMA) charts with control limits based on +/-3 standard deviations.
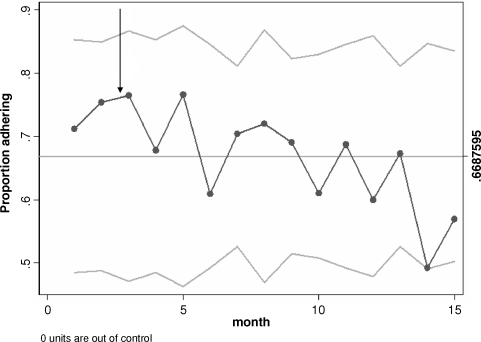
Results: A total of 1019 patients were referred to the centres during the study period. Monthly referrals overall increased by 40% following the introduction of eGFR reporting, and this was most marked for the tertiary renal service (52% above baseline). The appropriateness of nephrologist referrals, as adjudicated by the KCAT criteria, fell significantly from 74.3% in the 3 months pre-eGFR reporting to 65.2% in the 12 months thereafter (P < 0.05). Nevertheless, a greater absolute number of CKD patients were appropriately being referred for nephrologist review in the post-eGFR period (24 versus 15 per month). Patients referred following the introduction of eGFR were significantly more likely to be older (median 63.2 versus 59.3 years, P < 0.05), diabetic (25 versus 18%, P = 0.05) and have stage 3 CKD (48% versus 36%, P < 0.01).
Conclusion: The introduction of automated eGFR calculation has led to an overall increase in referrals with a small but significant decrease in referral quality. The increase in referrals was seen predominantly in older and diabetic patients with stage 3 CKD and appeared to result in net benefit.
Figures
References
-
- Weiner DE, Tighiouart H, Amin MG, et al. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004;15:1307–1315. - PubMed
-
- Dunstan D, Zimmet P, Welborn T, et al. AusDiab 2001: The Australian Diabetes, Obesity and Lifestyle Study. Melbourne: International Diabetes Institute; 2001.
-
- Dunstan D, Zimmet P, Welborn T, et al. AusDiab 2005: The Australian, Diabetes, Obesity and Lifestyle Study. Melbourne: International Diabetes Institute; 2005.
-
- El Nahas M. The global challenge of chronic kidney disease. Kidney Int. 2005;68:2918–2929. - PubMed
-
- Cass A, Cunningham J, Wang Z, et al. Social disadvantage and variation in the incidence of end-stage renal disease in Australian capital cities. Aust NZ J Public Health. 2001;25:322–326. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
