

Renal lesions associated with IgM-secreting monoclonal proliferations: revisiting the disease spectrum
- PMID: 18632851
- PMCID: PMC2518806
- DOI: 10.2215/CJN.01600408
Renal lesions associated with IgM-secreting monoclonal proliferations: revisiting the disease spectrum
Abstract
Background and objectives: Since the first description of pathology of the kidney in Waldenström disease in 1970, there have been few reports on kidney complications of IgM-secreting monoclonal proliferations. Here, we aimed to revisit the spectrum of renal lesions occurring in patients with a serum monoclonal IgM.
Design, setting, participants, & measurements: Fourteen patients with a circulating monoclonal IgM and a kidney disease related to B cell proliferation were identified retrospectively. Demographic, clinical, and laboratory data were assessed for each patient at the time of kidney biopsy.
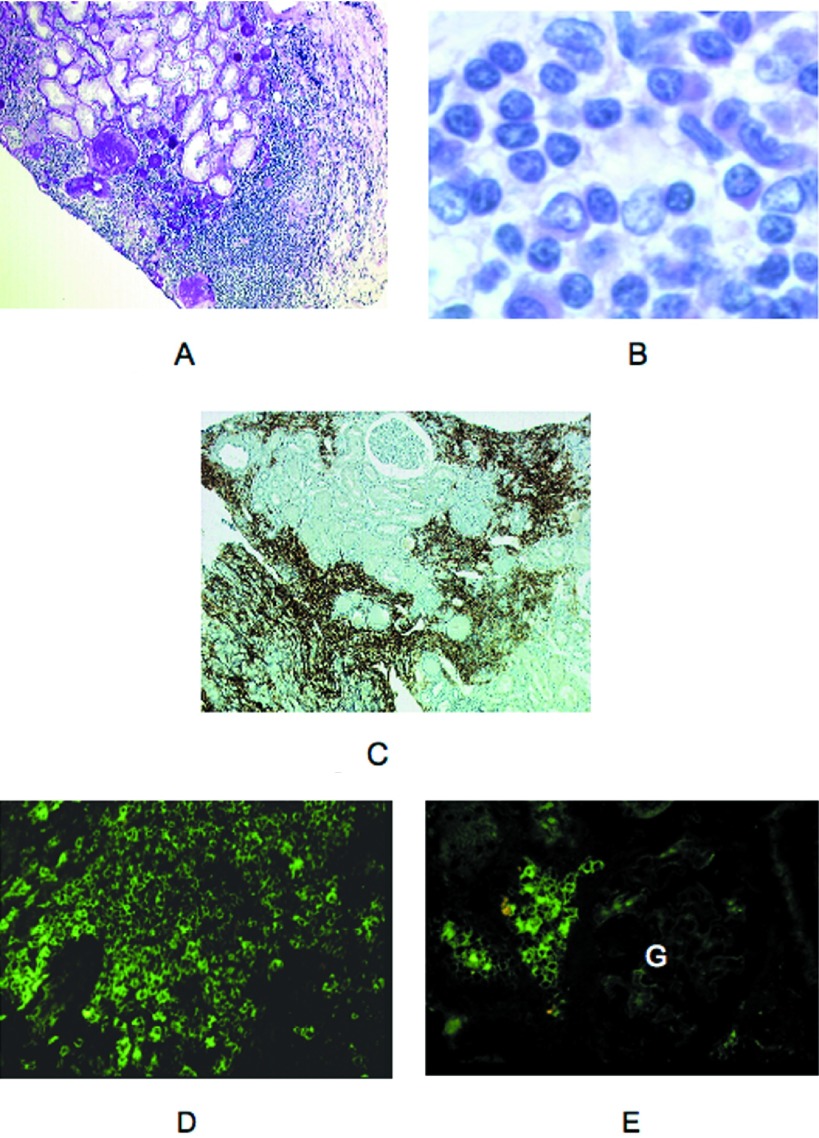
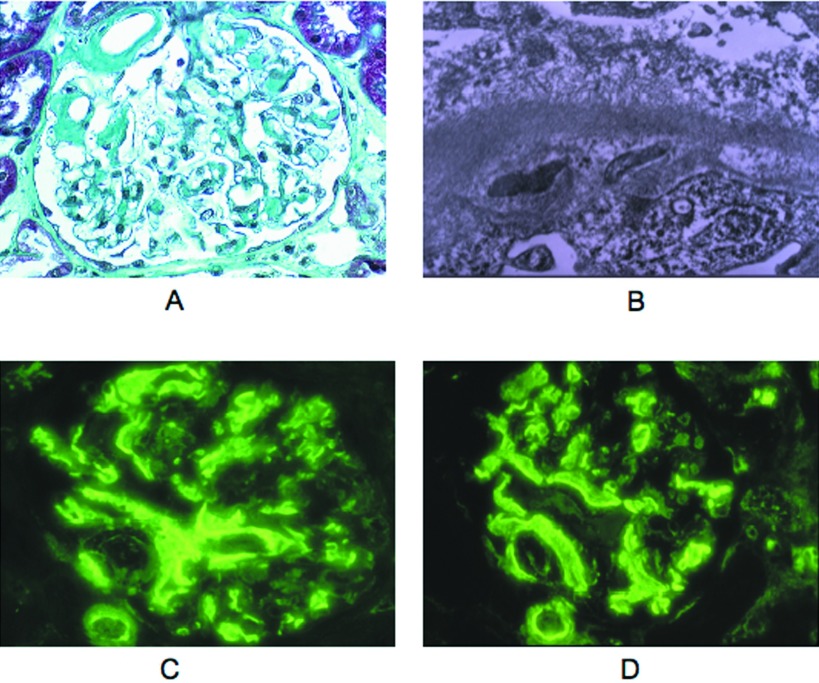
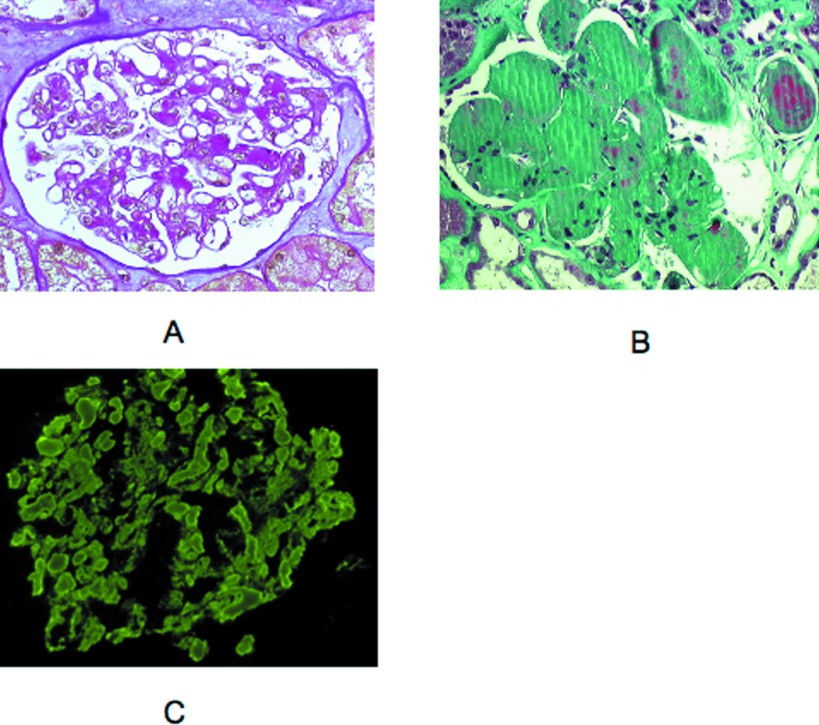
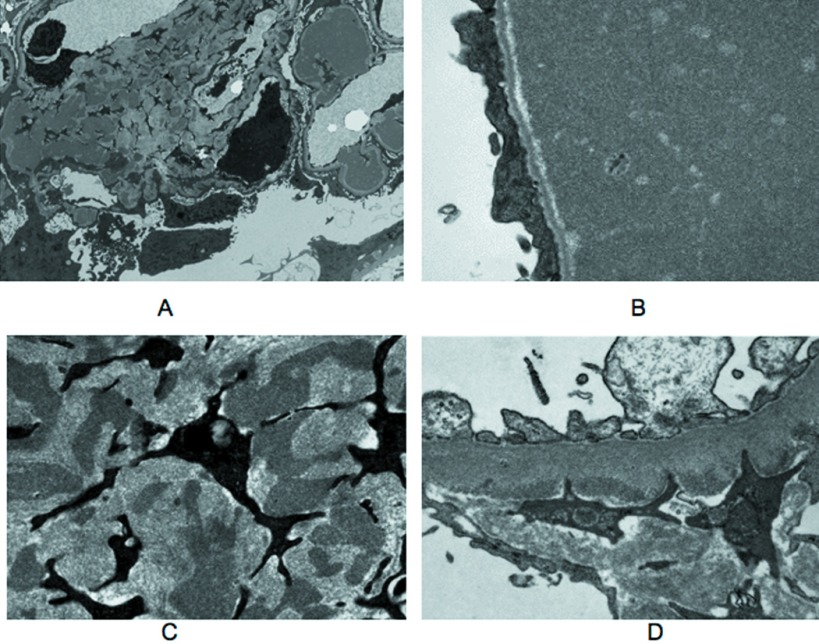
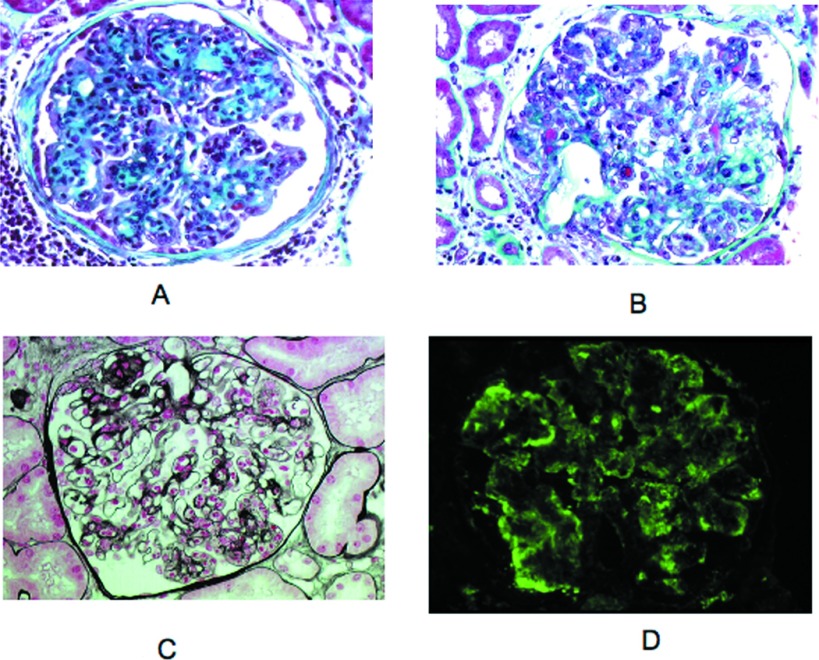
Results: Seven patients had a nephrotic syndrome. Patients without nephrotic syndrome all had impaired renal function. Mean serum creatinine was 238 micromol/L. For five patients, the diagnosis of monoclonal IgM preceded the kidney disease by 28.8 mo (range 12 to 60). Seven patients had Waldenström disease, two had a small B cell non-Hodgkin lymphoma, one had an IgM-excreting multiple myeloma, one had a marginal zone B cell lymphoma, and three had an IgM-related disorder. Renal lesions included (1) intracapillary monoclonal deposits disease with granular, electron-dense IgM thrombi occluding capillary lumens (5); (2) atypical membranoproliferative glomerulonephritis (3); (3) lambda light chain amyloidosis (2) associated with mu deposits in one patient; (4) acute tubular necrosis (1); and (5) CD20(+) lymphomatous infiltration (3). Remission of the nephrotic syndrome was attained in three of seven patients, and renal function improved after chemotherapy.
Conclusions: Although renal complications of IgM proliferations are rare, a wide spectrum of kidney lesions is observed, without correlation with the type of hematologic disorder.
Figures
References
-
- Solomon A, Weiss DT, Kattine AA: Nephrotoxic potential of Bence Jones proteins. N Engl J Med 324 :1845 –1851,1991 - PubMed
-
- Ronco P, Aucouturier P, Mougenot B: Monoclonal gammopathies: Multiple myeloma, amyloidosis, and related disorders. In: Diseases of the Kidney and Urinary Tract, 8th Ed., edited by Schrier RW, Philadelphia, Lippincott Williams & Wilkins,2007. , pp1941 –1985
-
- Morel-Maroger L, Basch A, Danon F, Verroust P, Richet G: Pathology of the kidney in Waldenström's macroglobulinemia: Study of sixteen cases. N Engl J Med 283 :123 –129,1970 - PubMed
-
- Da'as N, Kleinman Y, Polliack A, Amir G, Ne'eman Z, Kopolovic J, Bits H, Darmon D: Immunotactoid glomerulopathy with massive bone marrow deposits in a patient with IgM kappa monoclonal gammopathy and hypocomplementemia. Am J Kidney Dis 38 :395 –399,2001 - PubMed
-
- Dussol B, Kaplanski G, Daniel L, Brunet P, Pellissier JF, Berland Y: Simultaneous occurrence of fibrillary glomerulopathy and AL amyloid. Nephrol Dial Transplant 13 :2630 –2632,1998 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
