

Diagnosis of central nervous system tuberculosis by T-cell-based assays on peripheral blood and cerebrospinal fluid mononuclear cells
- PMID: 18632925
- PMCID: PMC2546678
- DOI: 10.1128/CVI.00040-08
Diagnosis of central nervous system tuberculosis by T-cell-based assays on peripheral blood and cerebrospinal fluid mononuclear cells
Abstract
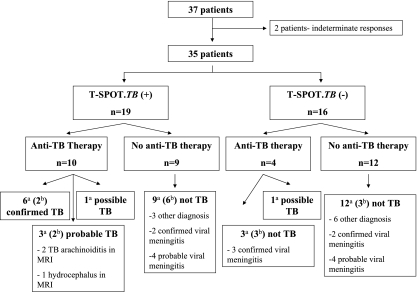
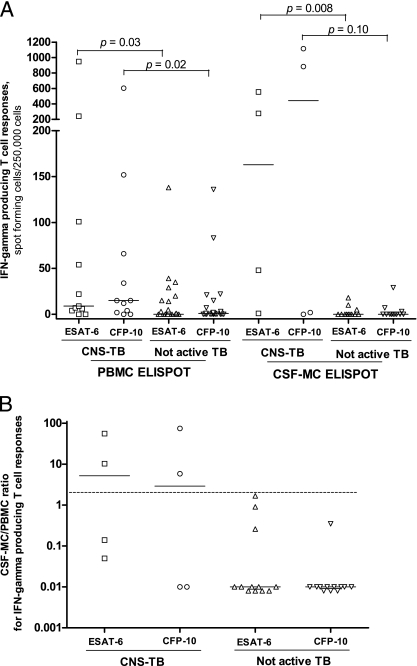
In active tuberculosis (TB), Mycobacterium tuberculosis-specific T cells are compartmentalized more to the site of infection than to the circulating blood. Therefore, an M. tuberculosis-specific enzyme-linked immunospot (ELISPOT) assay with samples from the site of infection may permit a more sensitive or specific diagnosis of active central nervous system (CNS) TB than that achieved by the assay with blood alone. Therefore, we prospectively evaluated the usefulness of circulating and compartmentalized mononuclear cell (MC; i.e., peripheral blood mononuclear cell [PBMC] and cerebrospinal fluid [CSF] MC)-based ELISPOT assays (i.e., the T-SPOT.TB test) for the diagnosis of active TB in patients with suspected CNS TB. The clinical categories of CNS TB were classified as described previously (G. E. Thwaites, T. T. Chau, K. Stepniewska, N. H. Phu, L. V. Chuong, D. X. Sinh, N. J. White, C. M. Parry, and J. J. Farrar, Lancet 360:1287-1292, 2002). Thirty-seven patients with suspected CNS TB were enrolled over a 12-month period. Of these, 31 (84%) showed clinical manifestations of suspected TB meningitis and 6 (16%) gave indications of intracranial tuberculoma with disseminated TB. The final clinical categories of the 37 patients with suspected CNS TB were as follows: 12 (32%) were classified as having CNS TB (7 with confirmed TB, 3 with probable TB, and 2 with possible TB) and 25 (68%) were classified as not having active TB. The sensitivity and specificity of the PBMC ELISPOT assay were 91% (95% confidence interval [CI], 59% to 100%) and 63% (95% CI, 41% to 81%), respectively. By comparison, the sensitivity and specificity of the CSF MC ELISPOT assay were 75% (95% CI, 19% to 99%) and 75% (95% CI, 43% to 95%), respectively. When the ratio of the CSF MC ELISPOT assay results to the PBMC ELISPOT results was 2 or more, the sensitivity and specificity were 50% (95% CI, 7% to 93%) and 100% (95% CI, 74% to 100%), respectively. The ELISPOT assay with PBMCs and CSF MCs is a useful adjunct to the current tests for the diagnosis of CNS TB.
Figures
References
-
- Baker, C. A., C. P. Cartwright, D. N. Williams, S. M. Nelson, and P. K. Peterson. 2002. Early detection of central nervous system tuberculosis with the Gen-Probe nucleic acid amplification assay: utility in an inner city hospital. Clin. Infect. Dis. 35:339-342. - PubMed
-
- Barry, S. M., M. C. Lipman, B. Bannister, M. A. Johnson, and G. Janossy. 2003. Purified protein derivative-activated type 1 cytokine-producing CD4+ T lymphocytes in the lung: a characteristic feature of active pulmonary and nonpulmonary tuberculosis. J. Infect. Dis. 187:243-250. - PubMed
-
- Breen, R. A., S. M. Barry, C. J. Smith, R. J. Shorten, J. P. Dilworth, I. Cropley, T. D. McHugh, S. H. Gillespie, G. Janossy, and M. C. Lipman. 2008. The clinical application of a rapid lung-orientated TB immunoassay in individuals with possible tuberculosis. Thorax 63:67-71. - PubMed
-
- Hirsch, C. S., Z. Toossi, J. L. Johnson, H. Luzze, P. Peters, M. McHugh, A. Okwera, M. Joloba, P. Mugyenyi, R. D. Mugerwa, P. Terebuh, and J. J. Ellner. 2001. Augmentation of apoptosis and interferon-gamma production at sites of active Mycobacterium tuberculosis infection in human tuberculosis. J. Infect. Dis. 183:779-788. - PubMed
-
- Jafari, C., M. Ernst, B. Kalsdorf, U. Greinert, R. Diel, D. Kirsten, K. Marienfeld, A. Lalvani, and C. Lange. 2006. Rapid diagnosis of smear-negative tuberculosis by bronchoalveolar lavage enzyme-linked immunospot. Am. J. Respir. Crit. Care Med. 174:1048-1054. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
