

Risk score and metastasectomy independently impact prognosis of patients with recurrent renal cell carcinoma
- PMID: 18635225
- PMCID: PMC2570431
- DOI: 10.1016/j.juro.2008.05.006
Risk score and metastasectomy independently impact prognosis of patients with recurrent renal cell carcinoma
Abstract
Purpose: We evaluated the prognostic roles of metastasectomy and an established risk stratification system in patients with disease recurrence following nephrectomy for nonmetastatic renal cell carcinoma.
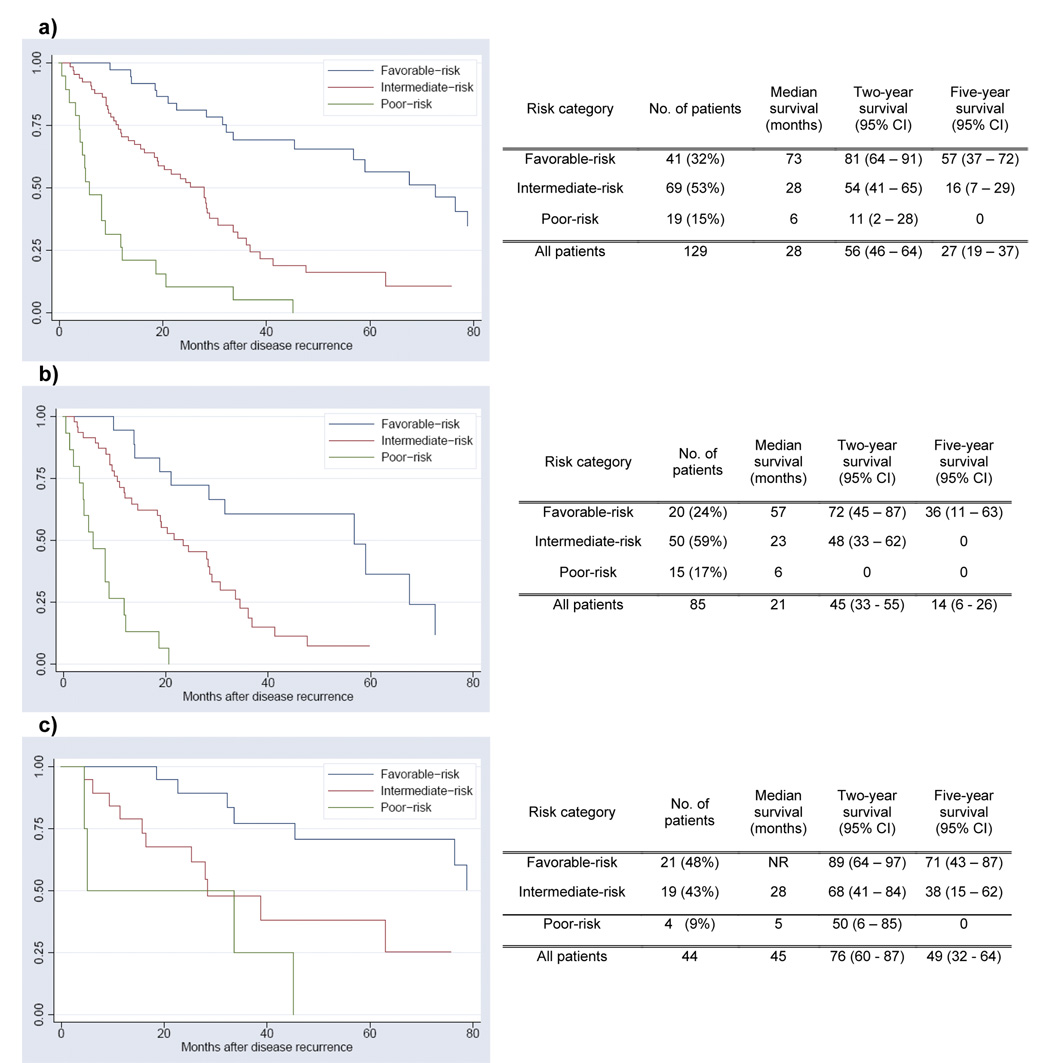
Materials and methods: A retrospective analysis was performed in 129 patients with localized renal cell carcinoma treated with partial or radical nephrectomy and subsequently diagnosed with disease recurrence. At recurrence a previously validated risk score based on Karnofsky performance status, interval from nephrectomy, and serum hemoglobin, calcium and lactate dehydrogenase was used to categorize patients as being at favorable, intermediate or poor risk. Survival from time of recurrence was assessed based on risk categorization and metastasectomy.
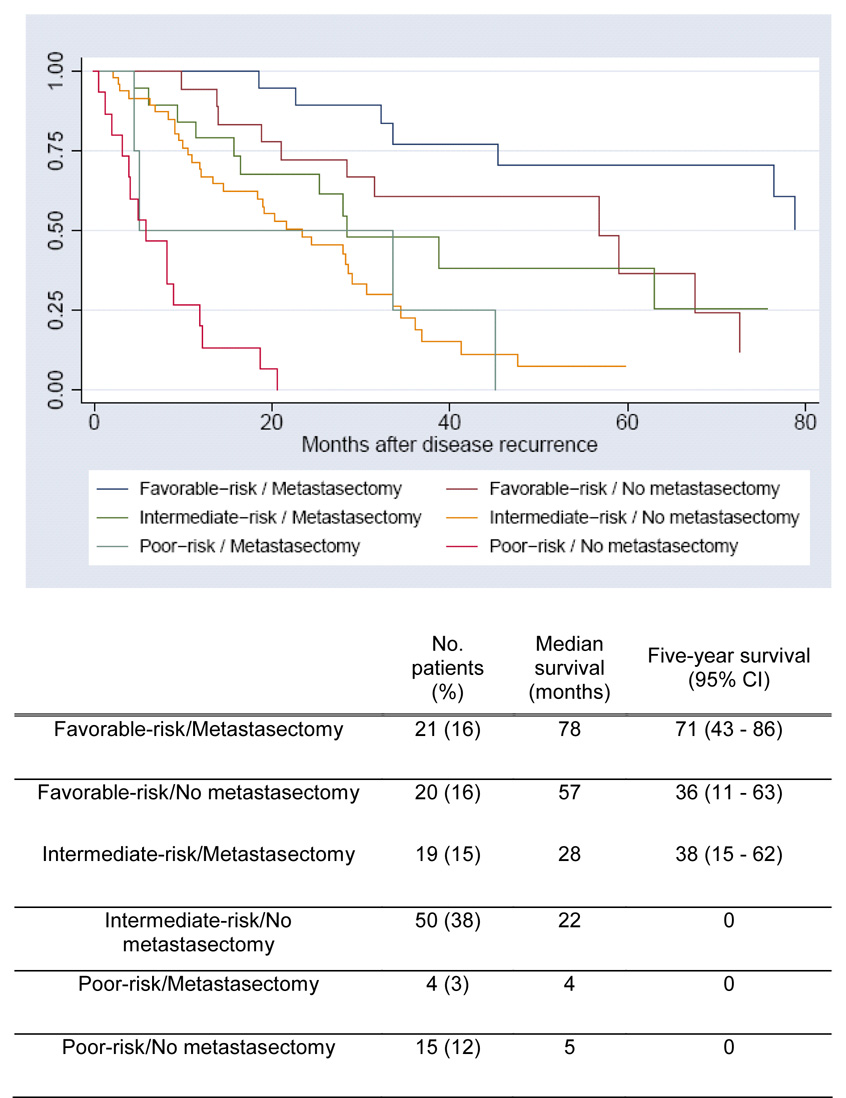
Results: Median time from nephrectomy to recurrence was 16 months. The risk score was strongly associated with median survival and the 2-year survival rate, including 73 months and 81% for favorable risk, 28 months and 54% for intermediate risk, and 6 months and 11% for poor risk, respectively (log rank <0.001). Metastasectomy performed in 44 patients (34%) was found to be of clinical benefit across the various risk categories (interaction analysis p = 0.8). On multivariate analysis a better risk category and metastasectomy were each independently associated with more favorable survival (each p <0.001). When combined, they provided 6 risk categories with an estimated 2-year survival of 0% to 93%.
Conclusions: The clinical course in patients with recurrent renal cell carcinoma following nephrectomy can be variable. It is independently impacted by an objectively determined risk score and whether the patient undergoes metastasectomy.
Conflict of interest statement
All authors report no potential conflicts of interest
Figures
References
-
- Cindolo L, Patard JJ, Chiodini P, Schips L, Ficarra V, Tostain J, et al. Comparison of predictive accuracy of four prognostic models for nonmetastatic renal cell carcinoma after nephrectomy: a multicenter European study. Cancer. 2005;104:1362. - PubMed
-
- Frank I, Blute ML, Cheville JC, Lohse CM, Weaver AL, Leibovich BC, et al. A multifactorial postoperative surveillance model for patients with surgically treated clear cell renal cell carcinoma. J Urol. 2003;170:2225. - PubMed
-
- Kattan MW, Reuter V, Motzer RJ, Katz J, Russo P. A postoperative prognostic nomogram for renal cell carcinoma. J Urol. 2001;166:63. - PubMed
-
- Lam JS, Shvarts O, Leppert JT, Pantuck AJ, Figlin RA, Belldegrun AS. Postoperative surveillance protocol for patients with localized and locally advanced renal cell carcinoma based on a validated prognostic nomogram and risk group stratification system. J Urol. 2005;174:466. - PubMed
-
- Lee CT, Katz J, Fearn PA, Russo P. Mode of presentation of renal cell carcinoma provides prognostic information. Urol Oncol. 2002;7:135. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
