

MR imaging: influence of imaging technique and postprocessing on measurement of internal carotid artery stenosis
- PMID: 18635618
- PMCID: PMC8118763
- DOI: 10.3174/ajnr.A1179
MR imaging: influence of imaging technique and postprocessing on measurement of internal carotid artery stenosis
Abstract
Background and purpose: MR angiography (MRA) is increasingly used as an alternative to digital subtraction angiography (DSA) to evaluate internal carotid artery (ICA) stenosis. Because MRA is not standardized in data acquisition and postprocessing, we sought to evaluate the effects of different acquisition techniques (time-of-flight MRA [TOF-MRA]) and contrast-enhanced MRA [CE-MRA]) and postprocessing methods (maximum intensity projection [MIP], multiplanar reformation [MPR], and volume-rendering on stenosis grading.
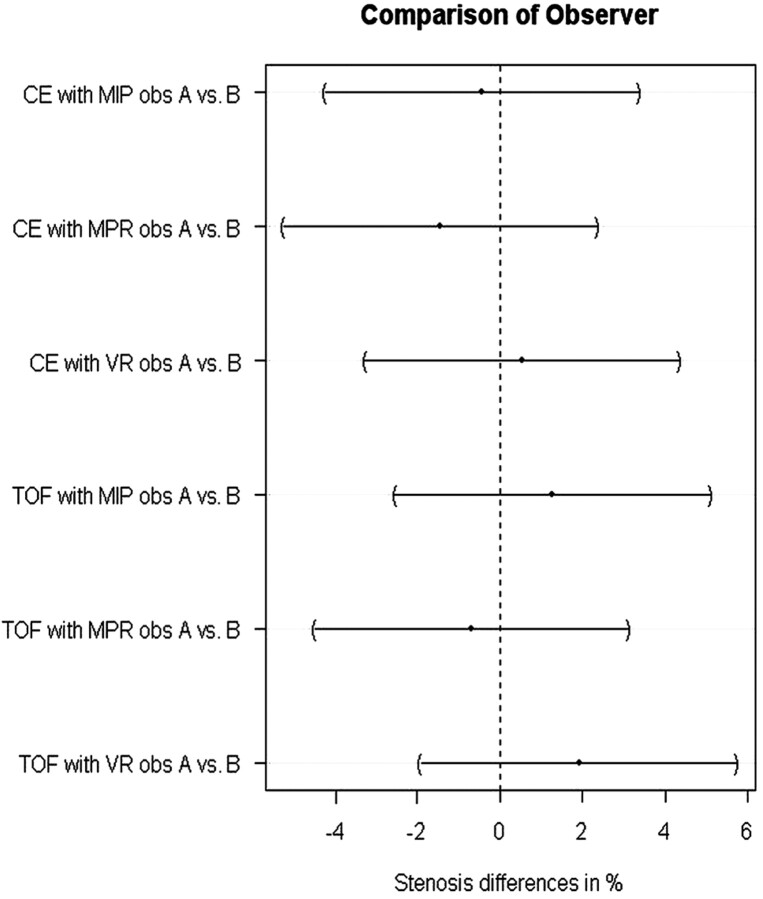
Materials and methods: Fifty patients (33 men, 17 women) with symptomatic ICA stenosis were examined at 1.5T. Two imaging techniques and 3 postprocessing methods resulted in 6 image datasets per patient. Two readers independently evaluated ICA stenosis according to the North American Symptomatic Carotid Endarterectomy Trial criteria. Interobserver variability was calculated with the Pearson correlation coefficient and simultaneous confidence intervals (CI). The relationship of the values of ICA stenosis between the techniques was assessed by means of simultaneous 95% Tukey CI.
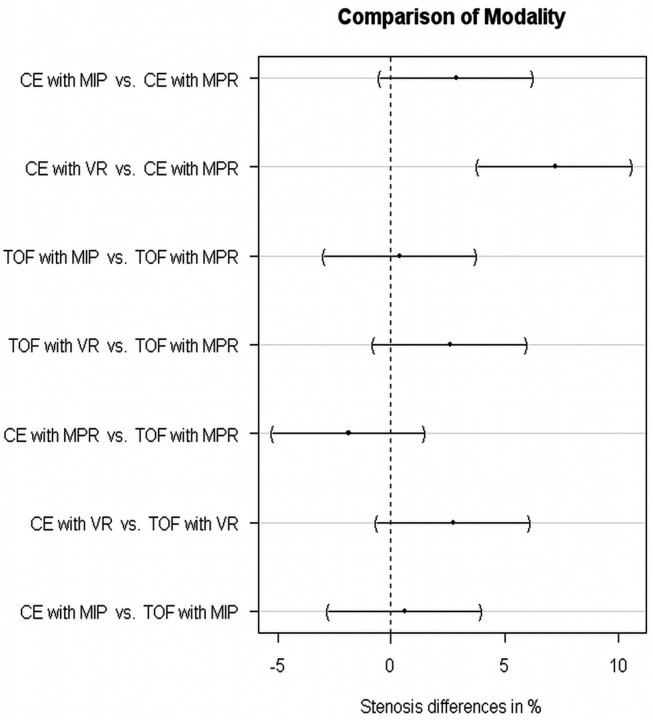
Results: Interobserver agreement was high. Higher concordance was found for postprocessing techniques with TOF- than with CE-MRA; the mean difference between TOF-MPR and TOF-MIP was 0.4% (95% CI, -2.9%-3.8%). Stenosis values for CE-MPR differed significantly from those of CE volume-rendering (7.2%; 95% CI, 3.9%-10.6%).
Conclusion: Stenosis grading was found to be independent of the postprocessing technique except for comparison of CE-MPR with CE volume-rendering, with the volume-rendering technique resulting in higher stenosis values. MPR seems to be best-suited for measurement of ICA stenosis. Parameter setting is critical with volume-rendering, in which stenosis values were consistently higher compared with the other methods.
Figures


Similar articles
-
Evaluation of carotid artery stenosis with multisection CT and MR imaging: influence of imaging modality and postprocessing.AJNR Am J Neuroradiol. 2007 Jan;28(1):104-10. AJNR Am J Neuroradiol. 2007. PMID: 17213434 Free PMC article.
-
MR angiography at 3 Tesla to assess proximal internal carotid artery stenoses: contrast-enhanced or 3D time-of-flight MR angiography?Clin Neuroradiol. 2015 Mar;25(1):41-8. doi: 10.1007/s00062-013-0279-x. Epub 2014 Jan 3. Clin Neuroradiol. 2015. PMID: 24384680
-
Grading of carotid artery stenosis in the presence of extensive calcifications: dual-energy CT angiography in comparison with contrast-enhanced MR angiography.Clin Neuroradiol. 2015 Mar;25(1):33-40. doi: 10.1007/s00062-013-0276-0. Epub 2013 Dec 17. Clin Neuroradiol. 2015. PMID: 24343701 Clinical Trial.
-
False-negative magnetic resonance angiography with extracranial internal carotid artery stenosis: a report of two cases and review of the literature.Neurosurg Rev. 2005 Apr;28(2):154-8. doi: 10.1007/s10143-004-0354-5. Epub 2004 Oct 8. Neurosurg Rev. 2005. PMID: 15480890 Review.
-
[Diagnosis of renal artery stenosis with magnetic resonance angiography and stenosis quantification].J Mal Vasc. 2000 Dec;25(5):312-320. J Mal Vasc. 2000. PMID: 11148391 Review. French.
Cited by
-
Improved carotid lumen delineation on non-contrast MR angiography using SNAP (Simultaneous Non-Contrast Angiography and Intraplaque Hemorrhage) imaging.Magn Reson Imaging. 2019 Oct;62:87-93. doi: 10.1016/j.mri.2019.06.012. Epub 2019 Jun 24. Magn Reson Imaging. 2019. PMID: 31247251 Free PMC article.
-
Assessment of carotid artery atherosclerotic disease by using three-dimensional fast black-blood MR imaging: comparison with DSA.Radiology. 2015 Feb;274(2):508-16. doi: 10.1148/radiol.14132687. Epub 2014 Oct 3. Radiology. 2015. PMID: 25286322 Free PMC article.
-
The added value of longitudinal black-blood cardiovascular magnetic resonance angiography in the cross sectional identification of carotid atherosclerotic ulceration.J Cardiovasc Magn Reson. 2009 Aug 18;11(1):31. doi: 10.1186/1532-429X-11-31. J Cardiovasc Magn Reson. 2009. PMID: 19689816 Free PMC article.
-
Feasibility of a sub-3-minute imaging strategy for ungated quiescent interval slice-selective MRA of the extracranial carotid arteries using radial k-space sampling and deep learning-based image processing.Magn Reson Med. 2020 Aug;84(2):825-837. doi: 10.1002/mrm.28179. Epub 2020 Jan 23. Magn Reson Med. 2020. PMID: 31975432 Free PMC article.
-
Contrast-enhanced MR angiography is not more accurate than unenhanced 2D time-of-flight MR angiography for determining > or = 70% internal carotid artery stenosis.AJNR Am J Neuroradiol. 2009 Apr;30(4):761-8. doi: 10.3174/ajnr.A1464. Epub 2009 Jan 22. AJNR Am J Neuroradiol. 2009. PMID: 19164440 Free PMC article.
References
-
- Rothwell PM, Eliasziw M, Gutnikov SA, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet 2003;361:107–16 - PubMed
-
- Endarterectomy for asymptomatic carotid artery stenosis: Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA 1995;273:1421–28 - PubMed
-
- Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet 1998;351:1379–87 - PubMed
-
- Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med 1998;339:1415–25 - PubMed
-
- Buskens E, Nederkoorn PJ, Buijs-Van Der Woude T, et al. Imaging of carotid arteries in symptomatic patients: cost-effectiveness of diagnostic strategies. Radiology 2004;233:101–12 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous