

No impairment of endothelial function or insulin sensitivity with 4 weeks of the HIV protease inhibitors atazanavir or lopinavir-ritonavir in healthy subjects without HIV infection: a placebo-controlled trial
- PMID: 18636958
- PMCID: PMC2919310
- DOI: 10.1086/590154
No impairment of endothelial function or insulin sensitivity with 4 weeks of the HIV protease inhibitors atazanavir or lopinavir-ritonavir in healthy subjects without HIV infection: a placebo-controlled trial
Abstract
Background: Dyslipidemia alone does not fully explain the increase in cardiovascular events among patients receiving protease inhibitor (PI)-based treatment for human immunodeficiency virus infection. Some PIs, such as indinavir, directly induce endothelial dysfunction, an effect that may mediate that portion of the increase in cardiovascular events that is not attributable to dyslipidemia.
Methods: Endothelium-dependent vasodilation, insulin-mediated vasodilation, and whole-body and leg glucose uptake during use of a 1-h euglycemic hyperinsulinemic clamp (insulin infusion, 40 mU/m(2)/min) were measured in healthy men before and after 4 weeks of treatment with placebo (12 men), with 400 mg atazanavir per day (9 men), or with 400 mg lopinavir and 100 mg ritonavir twice per day (9 men).
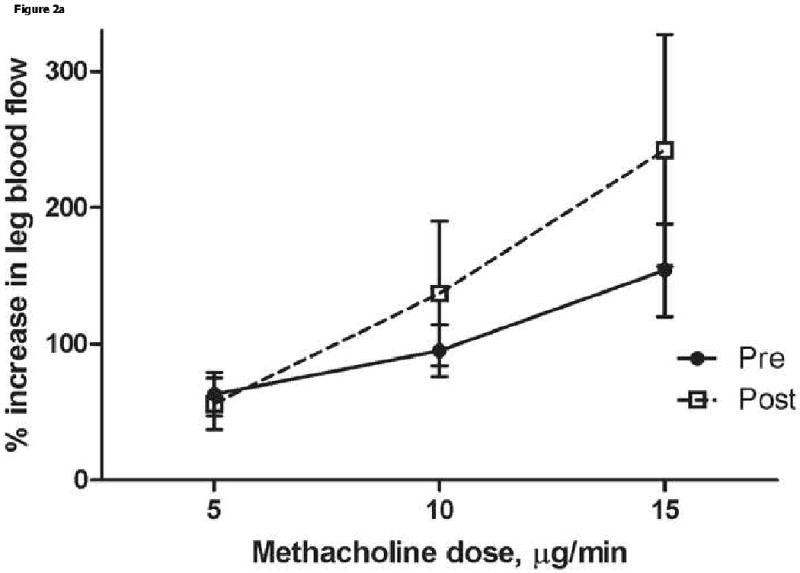
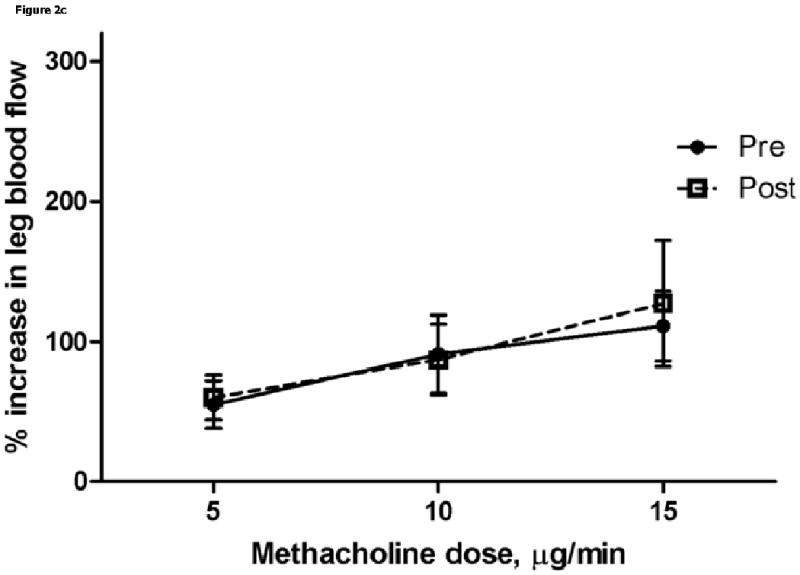
Results: Median age (36 years) and mean body mass index SD (23.4+/-2.6; calculated as weight in kilograms divided by the square of height in meters) did not differ between groups. Endothelium-dependent vasodilation, expressed as the percentage change in the leg blood flow response to intrafemoral artery infusion of 15 microg/min of the endothelium-dependent vasodilator methacholine, did not change after 4 weeks of treatment in any group:mean percentage change +/- SD, 154+/-102 from baseline and 242+/-254 at week 4 with atazanavir (P=.36), 76+/-62 and 86+/-79, respectively, with lopinavir-ritonavir (P=.68), and 111+/-86 and 127+/-153, respectively,with placebo (P=.63; for between-group differences, P=.55). The response to the endothelium-independent vasodilator nitroprusside was not different at week 4 for any group, nor was insulin-mediated vasodilation or leg or whole-body insulin-mediated glucose uptake (all within-group P values were 1.1).
Conclusions: Unlike the dramatic impairment seen with indinavir, the newer PIs atazanavir and lopinavir-ritonavir do not induce endothelial dysfunction in healthy subjects. Thus, endothelial dysfunction does not appear to be a PI drug class effect. The cause of the non-lipid-mediated increase in cardiovascular events that are reported with PIs remains unclear.
Conflict of interest statement
Figures


Comment in
-
Understanding the complications of antiretroviral drugs.Clin Infect Dis. 2008 Aug 15;47(4):575-6. doi: 10.1086/590155. Clin Infect Dis. 2008. PMID: 18611156 Free PMC article. No abstract available.
References
-
- D. A. D. Study Group. Friis-Moller N, Reiss P, et al. Class of antiretroviral drugs and the risk of myocardial infarction. New England Journal of Medicine. 2007;356:1723–35. - PubMed
-
- Mary-Krause M, Cotte L, Simon A, Partisani M, Costagliola D. Increased risk of myocardial infarction with duration of protease inhibitor therapy in HIV-infected men. AIDS. 2003;17:2479–86. - PubMed
-
- Celermajer DS. Endothelial dysfunction: Does it matter? Is it reversible? J Am Coll Cardiol. 1997;30:325–33. - PubMed
-
- Kinlay S, Ganz P. Role of endothelial dysfunction in coronary artery disease and implications for therapy. Am J Cardiol. 1997;80:11I–16I. - PubMed
-
- Stein JH, Klein MA, Bellehumeur JL, et al. Use of human immunodeficiency virus-1 protease inhibitors is associated with atherogenic lipoprotein changes and endothelial dysfunction. Circulation. 2001;104:257–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
