

Utilizing intraluminal pressure gradients to predict esophageal clearance: a validation study
- PMID: 18637086
- PMCID: PMC2887307
- DOI: 10.1111/j.1572-0241.2008.01913.x
Utilizing intraluminal pressure gradients to predict esophageal clearance: a validation study
Abstract
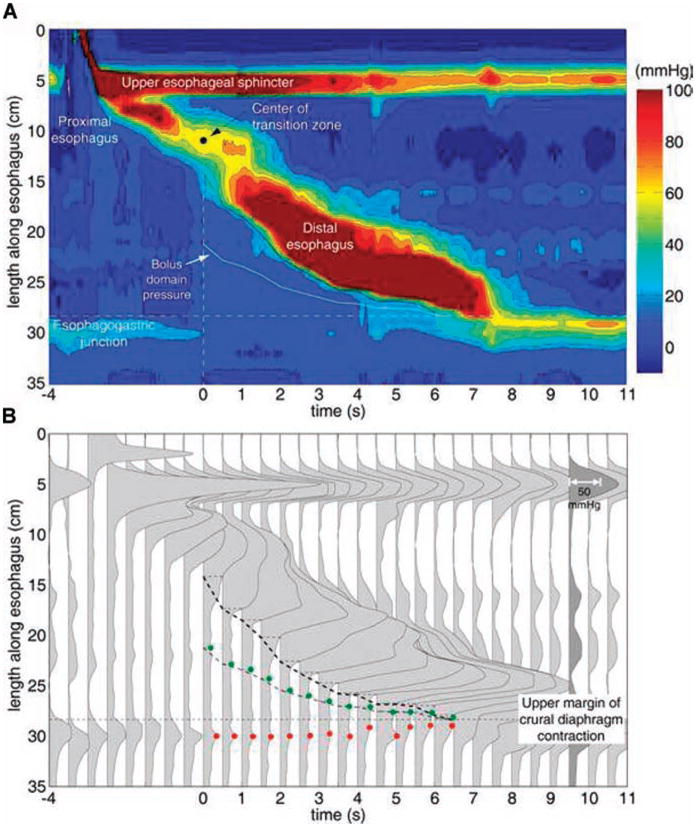
Background: Esophageal bolus clearance requires a preferential esophagogastric pressure gradient sustained for a sufficient period. We aimed to validate a high-resolution manometry (HRM) paradigm for predicting bolus clearance.
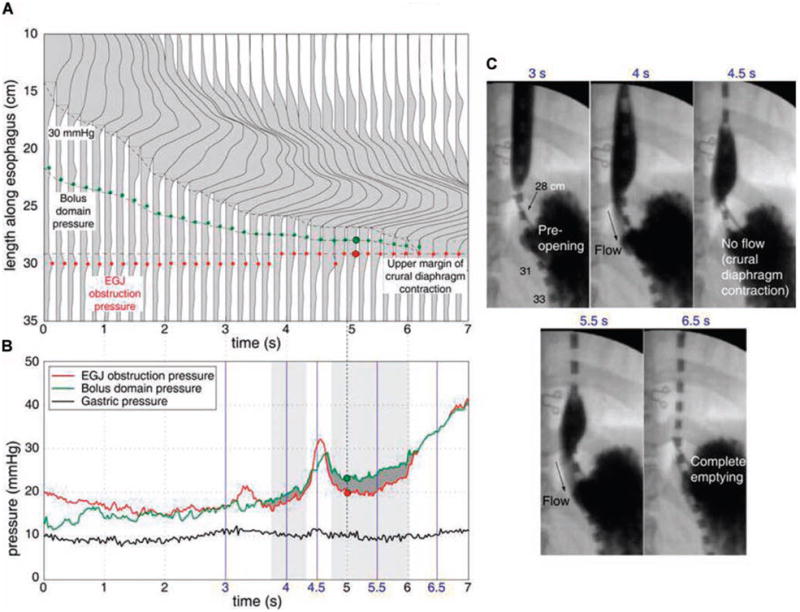
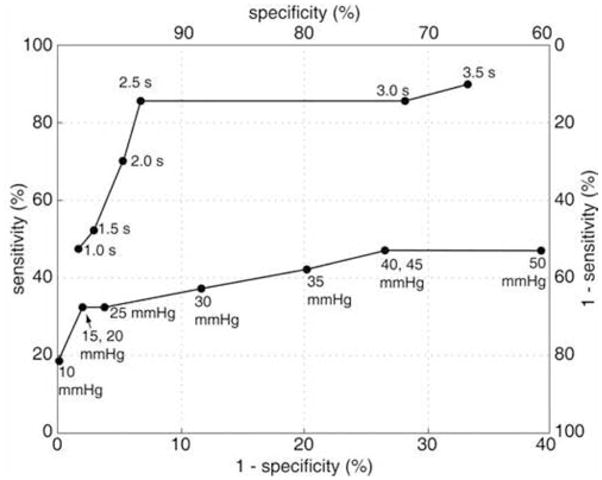
Methods: Twenty volunteers and 30 patients were studied with HRM during barium swallows with concurrent fluoroscopy. Simultaneous bolus domain pressure and esophagogastric junction (EGJ) obstruction pressure were plotted and flow permissive time was tallied during which the bolus domain pressure exceeded the EGJ obstruction pressure. Distal peristaltic integrity was assessed at incrementally increasing pressure isobaric contour thresholds from 15-40 mmHg. ROC analysis was performed to assess the sensitivity and specificity of cutoff values for flow permissive time and peristaltic amplitude for predicting incomplete clearance as verified fluoroscopically.
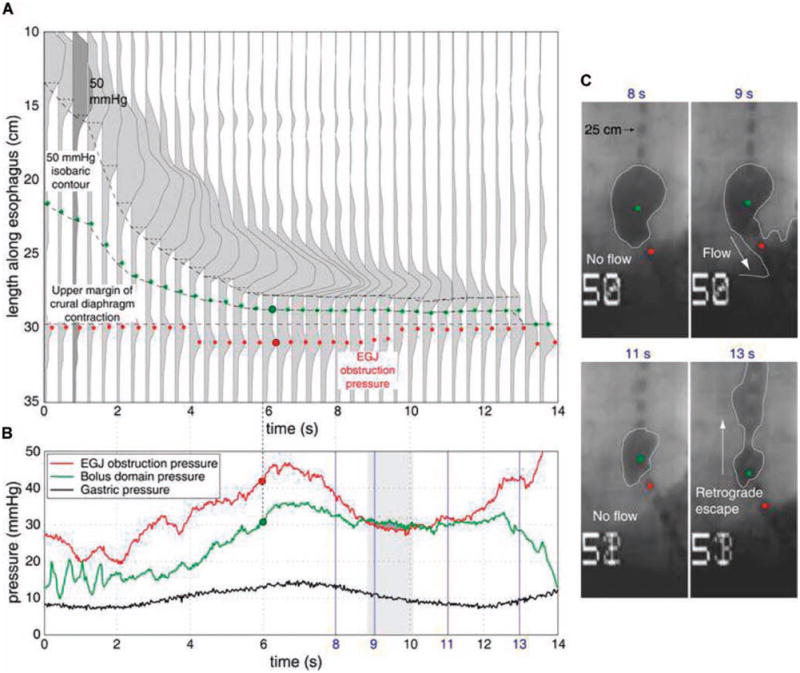
Results: Flow permissive time < or =2.5 s had a sensitivity of 86% and specificity of 92% for predicting incomplete clearance. In contrast, a 30-mmHg peristaltic amplitude had a sensitivity of only 48% and specificity of 88%. Incomplete clearance was variably attributable to functional EGJ obstruction, hiatus hernia, or impaired peristalsis.
Conclusions: A detailed analysis of intraluminal pressure gradients in the distal esophagus and across the EGJ in the postdeglutitive period predicts esophageal bolus clearance with far greater accuracy than any threshold value of peristaltic amplitude.
Conflict of interest statement
Figures

References
-
- Fox M, Hebbard G, Janiak P, et al. High-resolution manometry predicts the success of oesophageal bolus transport and identifies clinically important abnormalities not detected by conventional manometry. Neurogastroenterol Motil. 2004;16:533–42. - PubMed
-
- Ghosh SK, Kahrilas PJ, Lodhia N, et al. Utilizing intraluminal pressure differences to predict esophageal bolus flow dynamics. Am J Physiol Gastrointest Liver Physiol. 2007;293:G1023–8. - PubMed
-
- Pandolfino JE, El-Serag HB, Zhang Q, et al. Obesity: A challenge to esophagogastric junction integrity. Gastroenterology. 2006;130:639–49. - PubMed
-
- Clouse RE, Staiano A. Topography of the esophageal peristaltic pressure wave. Am J Physiol. 1991;261:G677–84. - PubMed
-
- Ghosh SK, Pandolfino JE, Zhang Q, et al. Quantifying esophageal peristalsis with high-resolution manometry: A study of 75 asymptomatic volunteers. Am J Physiol Gastrointest Liver Physiol. 2006;290:G988–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
