

Sex and socioeconomic differentials in child health in rural Bangladesh: findings from a baseline survey for evaluating Integrated Management of Childhood Illness
- PMID: 18637525
- PMCID: PMC2740675
Sex and socioeconomic differentials in child health in rural Bangladesh: findings from a baseline survey for evaluating Integrated Management of Childhood Illness
Abstract
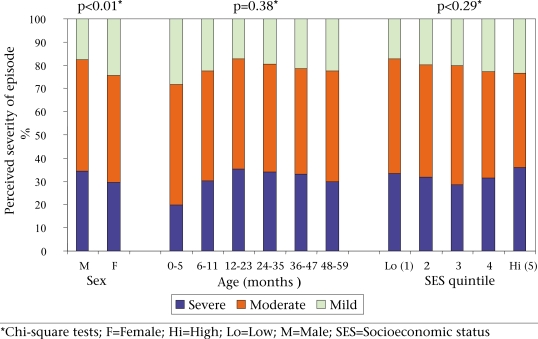
This paper reports on a population-based sample survey of 2,289 children aged less than five years (under-five children) conducted in 2000 as a baseline for the Bangladesh component of the Multi-country Evaluation (MCE) of the Integrated Management of Childhood Illness strategy. Of interest were rates and differentials by sex and socioeconomic status for three aspects of child health in rural Bangladesh: morbidity and hospitalizations, including severity of illness; care-seeking for childhood illness; and home-care for illness. The survey was carried out among a population of about 380,000 in Matlab upazila (subdistrict). Generic MCE Household Survey tools were adapted, translated, and pretested. Trained interviewers conducted the survey in the study areas. In total, 2,289 under-five children were included in the survey. Results showed a very high prevalence of illness among Bangladeshi children, with over two-thirds reported to have had at least one illness during the two weeks preceding the survey. Most sick children in this population had multiple symptoms, suggesting that the use of the IMCI clinical guidelines will lead to improved quality of care. Contrary to expectations, there were no significant differences in the prevalence of illness either by sex or by socioeconomic status. About one-third of the children with a reported illness did not receive any care outside the home. Of those for whom outside care was sought, 42% were taken to a village doctor. Only 8% were taken to an appropriate provider, i.e. a health facility, a hospital, a doctor, a paramedic, or a community-based health worker. Poorer children than less-poor children were less likely to be taken to an appropriate healthcare provider. The findings indicated that children with severe illness in the least poor households were three times more likely to seek care from a trained provider than children in the poorest households. Any evidence of gender inequities in child healthcare, either in terms of prevalence of illness or care-seeking patterns, was not found. Care-seeking patterns were associated with the perceived severity of illness, the presence of danger signs, and the duration and number of symptoms. The results highlight the challenges that will need to be addressed as IMCI is implemented in health facilities and extended to address key family and community practices, including extremely low rates of use of the formal health sector for the management of sick children. Child health planners and researchers must find ways to address the apparent population preference for untrained and traditional providers which is determined by various factors, including the actual and perceived quality of care, and the differentials in care-seeking practices that discriminate against the poorest households.
Figures


References
-
- UNICEF statistical database (www.childinfo.org-cmr-revis-db2_files, accessed on 2 December 2002).
-
- Bangladesh demographic and health survey 1999–2000. Dhaka: National Institute of Population Research and Training; 2001. National Institute of Population Research and Training; pp. 100–6.
-
- Mitra SN, Ali MN, Islam S, Cross AR, Saha T. Dhaka: National Institute of Population Research and Training; 1994. Bangladesh demographic and health survey, 1993–1994; pp. 39–40.
-
- Mitra SN, Al-Sabir A, Cross AR, Jamil K. Dhaka: National Institute of Population Research and Training; 1997. Bangladesh demographic and health survey, 1996–1997; pp. 99–102.
-
- Health and demographic surveillance system—Matlab. V. 33. Registration of health and demographic events 2000. Dhaka: International Centre for Diarrhoeal Disease Research, Bangladesh; 2002. International Centre for Diarrhoeal Disease Research, Bangladesh; p. 102. (ICDDR,B scientific report no. 89)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical