

Post-mortem clinical pharmacology
- PMID: 18637886
- PMCID: PMC2561112
- DOI: 10.1111/j.1365-2125.2008.03231.x
Post-mortem clinical pharmacology
Abstract
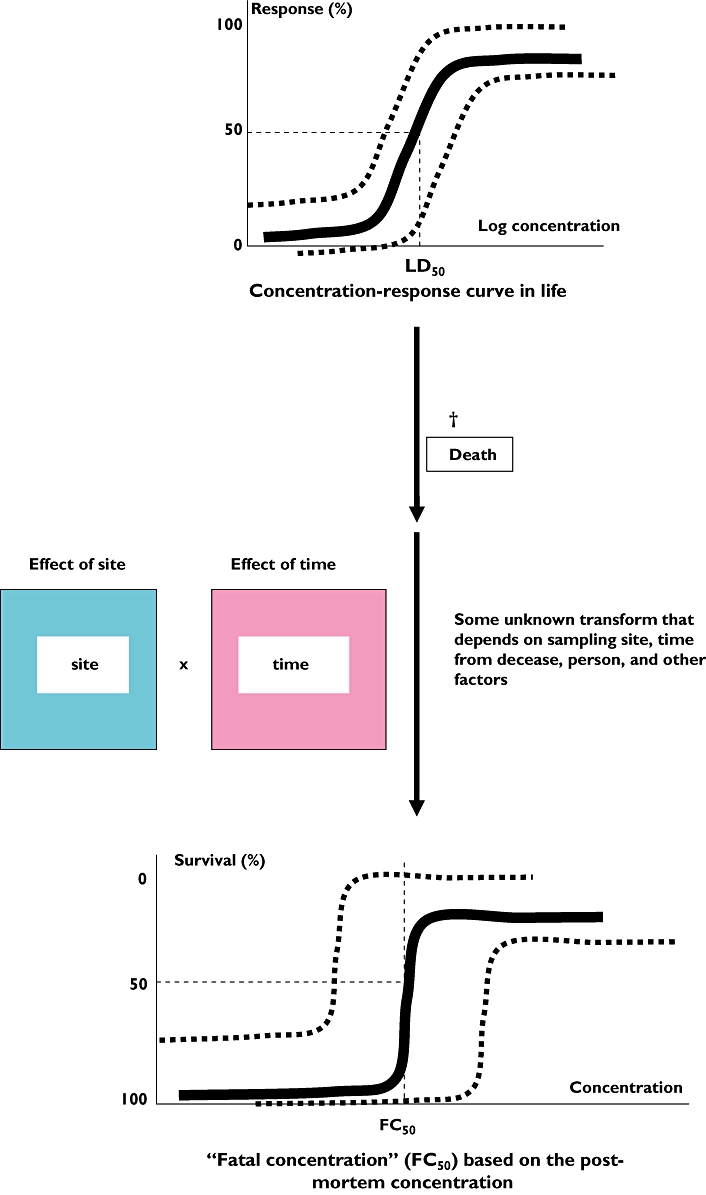
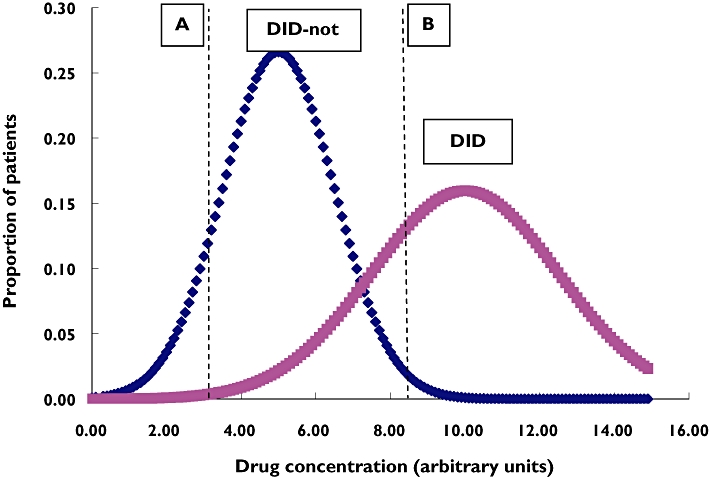
Clinical pharmacology assumes that deductions can be made about the concentrations of drugs from a knowledge of the pharmacokinetic parameters in an individual; and that the effects are related to the measured concentration. Post-mortem changes render the assumptions of clinical pharmacology largely invalid, and make the interpretation of concentrations measured in post-mortem samples difficult or impossible. Qualitative tests can show the presence of substances that were not present in life, and can fail to detect substances that led to death. Quantitative analysis is subject to error in itself, and because post-mortem concentrations vary in largely unpredictable ways with the site and time of sampling, as a result of the phenomenon of post-mortem redistribution. Consequently, compilations of 'lethal concentrations' are misleading. There is a lack of adequate studies of the true relationship between fatal events and the concentrations that can be measured subsequently, but without such studies, clinical pharmacologists and others should be wary of interpreting post-mortem measurements.
Figures



Comment in
-
Prediction and reverse prediction in therapeutics and toxicology.Br J Clin Pharmacol. 2008 Oct;66(4):427-9. doi: 10.1111/j.1365-2125.2008.03293.x. Br J Clin Pharmacol. 2008. PMID: 18826518 Free PMC article. No abstract available.
References
-
- Ferner RE. Forensic Pharmacology: Medicines, Mayhem, and Malpractice. Oxford: Oxford University Press; 1996.
-
- Koniaris LG, Zimmers TA, Lubarsky DA, Sheldon JP. Inadequate anaesthesia in lethal injection for execution. Lancet. 2005;365:1412–14. - PubMed
-
- Heath MJS, Stanski DR, Pounder DJ. Inadequate anaesthesia in lethal injection for execution. Lancet. 2005;366:1073–4. - PubMed
-
- Drummer OH, Gerostamoulos J. Postmortem drug analysis: analytical and toxicological aspects. Ther Drug Monit. 2002;24:199–209. - PubMed
-
- Flanagan RJ, Connally G. Interpretation of analytical toxicology results in life and at postmortem. Toxicol Rev. 2005;24:51–6. - PubMed
