

Health care costs, long-term survival, and quality of life following intensive care unit admission after cardiac arrest
- PMID: 18638367
- PMCID: PMC2575575
- DOI: 10.1186/cc6963
Health care costs, long-term survival, and quality of life following intensive care unit admission after cardiac arrest
Abstract
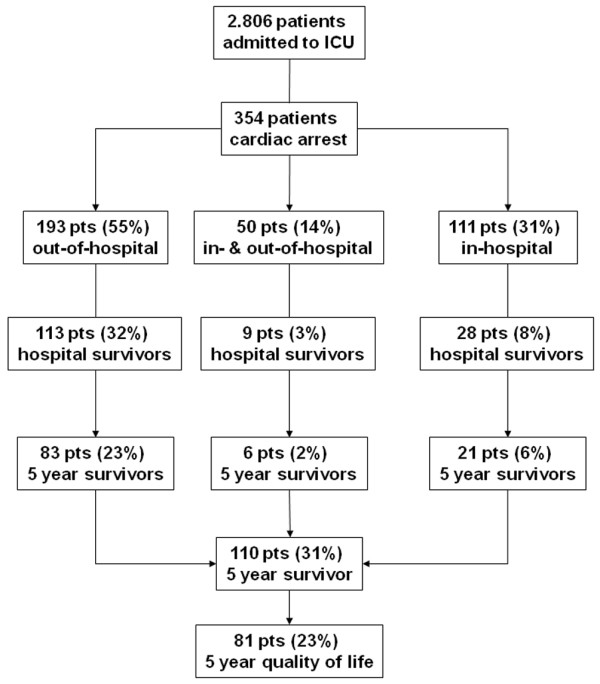
Introduction: The purpose of this study was to investigate the costs and health status outcomes of intensive care unit (ICU) admission in patients who present after sudden cardiac arrest with in-hospital or out-of-hospital cardiopulmonary resuscitation.
Methods: Five-year survival, health-related quality of life (Medical Outcome Survey Short Form-36 questionnaire, SF-36), ICU costs, hospital costs and post-hospital health care costs per survivor, costs per life year gained, and costs per quality-adjusted life year gained of patients admitted to a single ICU were assessed.
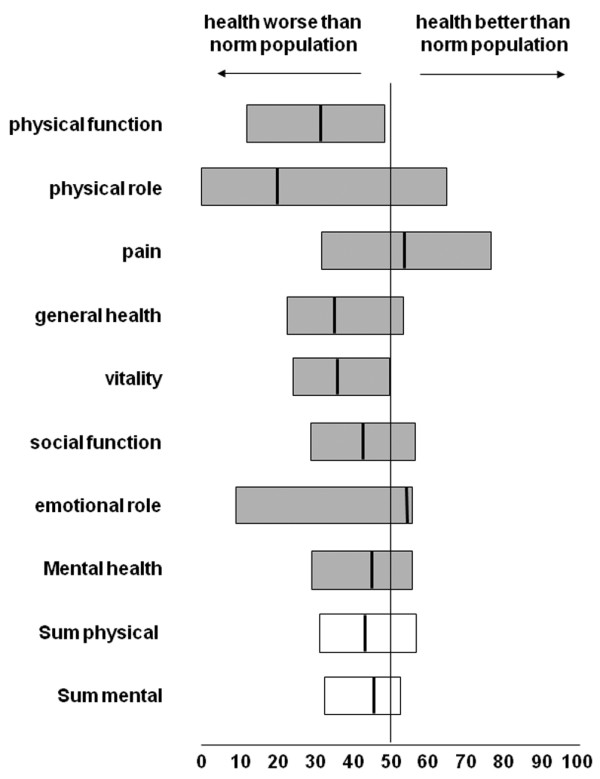
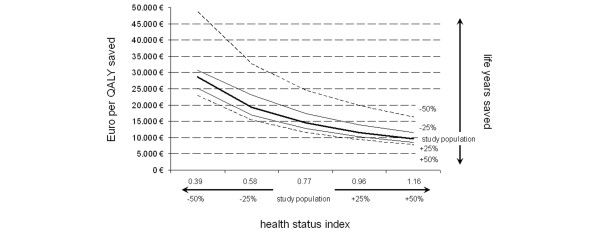
Results: One hundred ten of 354 patients (31%) were alive 5 years after hospital discharge. The mean health status index of 5-year survivors was 0.77 (95% confidence interval 0.70 to 0.85). Women rated their health-related quality of life significantly better than men did (0.87 versus 0.74; P < 0.05). Costs per hospital discharge survivor were 49,952 euro. Including the costs of post-hospital discharge health care incurred during their remaining life span, the total costs per life year gained were 10,107 euro. Considering 5-year survivors only, the costs per life year gained were calculated as 9,816 euro or 14,487 euro per quality-adjusted life year gained. Including seven patients with severe neurological sequelae, costs per life year gained in 5-year survivors increased by 18% to 11,566 euro.
Conclusion: Patients who leave the hospital following cardiac arrest without severe neurological disabilities may expect a reasonable quality of life compared with age- and gender-matched controls. Quality-adjusted costs for this patient group appear to be within ranges considered reasonable for other groups of patients.
Figures
Comment in
-
A call to arms to reduce premature deaths by using inexpensive resuscitation care.Crit Care. 2008;12(4):173. doi: 10.1186/cc6970. Epub 2008 Aug 19. Crit Care. 2008. PMID: 18771587 Free PMC article.
References
-
- Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage. JAMA. 1960;173:1064–1067. - PubMed
-
- Kuckelt W. Notes in intensive care medicine in Europe. Intensive care medicine in Germany. In: Reis Miranda D, Ryan DW, Schaufeli WB, Fidler V, editor. Organisation and Management of Intensive Care A Prospective Study in 12 European Countries. Berlin: Springer; 1998. pp. 88–90.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
