

Histopathological assessment of prostate cancer bone osteoblastic metastases
- PMID: 18639279
- PMCID: PMC2992811
- DOI: 10.1016/j.juro.2008.04.140
Histopathological assessment of prostate cancer bone osteoblastic metastases
Abstract
Purpose: Many patients with prostate cancer have bone metastases that appear osteoblastic on radiography, and yet these patients are at increased risk for fracture. The discrepancy between the radiological and clinical aspects of those events is not well understood. We better characterized the histopathology of bone processes in prostate cancer bone metastases.
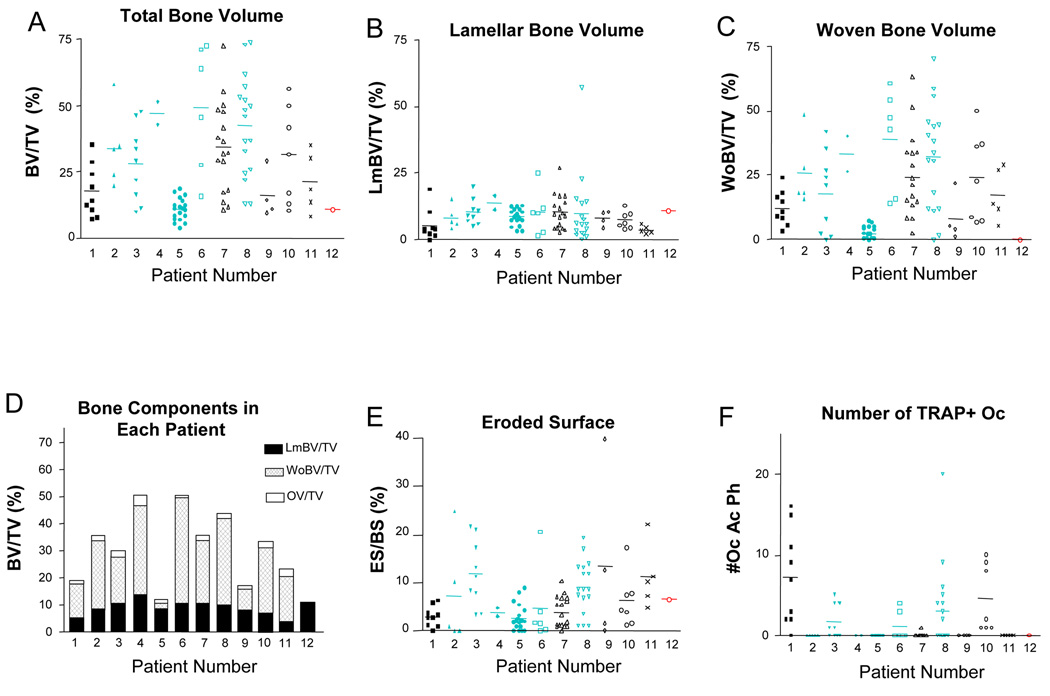
Materials and methods: Histomorphometry was used to evaluate multisite bone biopsies in 12 patients who died with multiple bone metastases, of whom 7 had received bisphosphonate therapy.
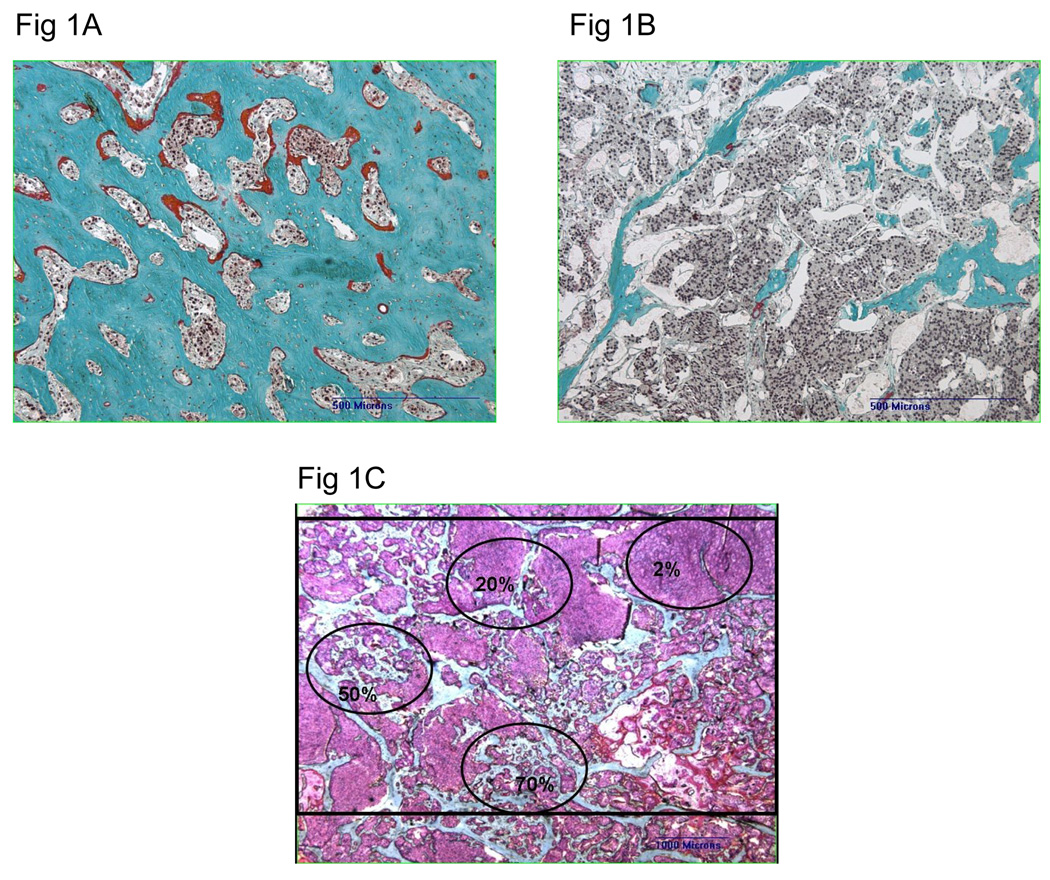
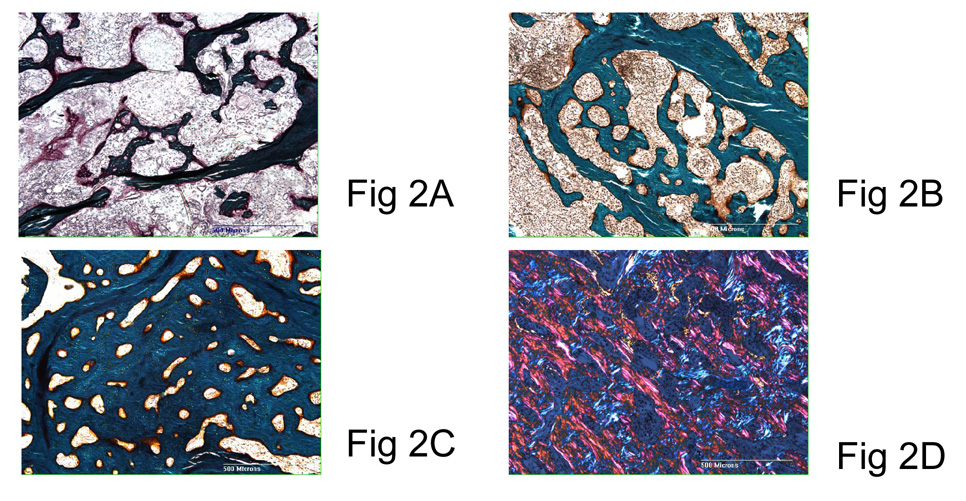
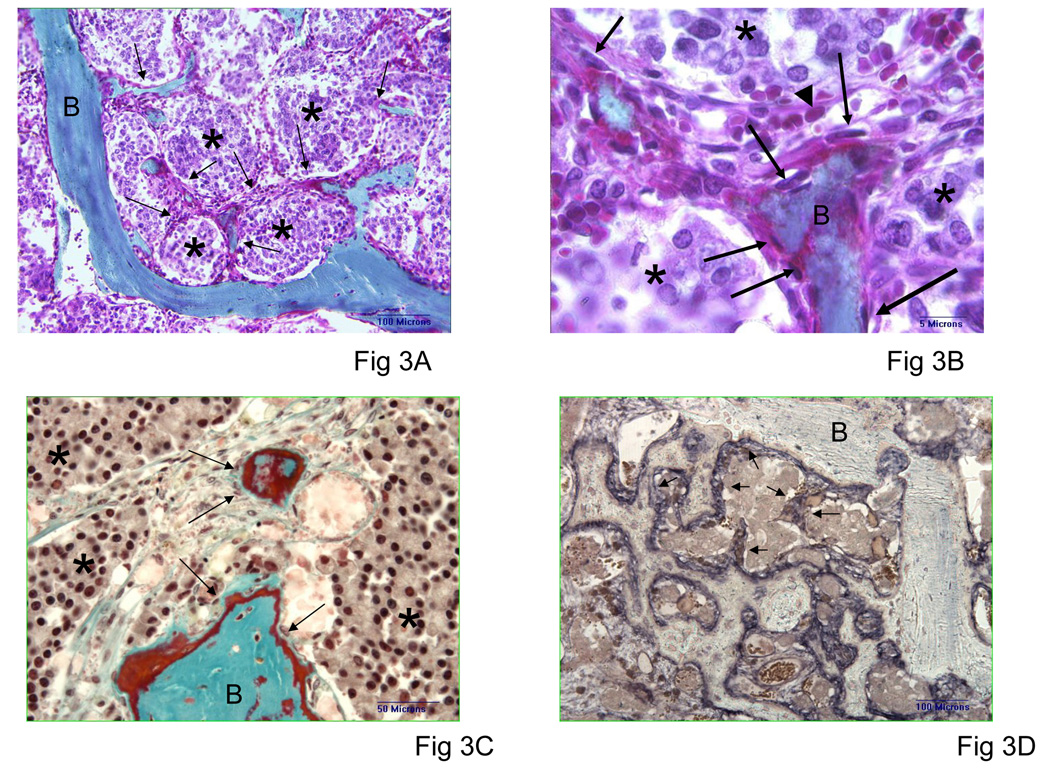
Results: Bone histomorphometry revealed a wide spectrum of cancer induced bone changes in different metastatic sites in individual patients, ranging from a pronounced osteodense to a pronounced osteopenic type. Each metastatic lesion was associated with various amounts of resorption. Decreased bone volume was seen in half of all biopsies. Osteodense lesions were largely composed of under mineralized woven bone, which increases the frailty of new bone. Interestingly woven bone was produced by alkaline phosphatase spindle-shaped cells arising from the connective stroma surrounding tumor cells. The bone response generally was similar in bisphosphonate treated patients and those who did not receive bisphosphonate.
Conclusions: Despite the osteoblastic nature of bone metastases in prostate cancer, the osteolytic-osteopenic bone lesions found in each clinically osteoblastic case may explain the frequent fractures observed in these cases. In addition, the finding that woven bone formed directly from the tumor stroma and not from the adjacent bone surface supports further research into the mechanisms of abnormal bone formation in prostate cancer bone metastases.
Figures


References
-
- Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, et al. Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: the effect of bisphosphonate therapy on bone scintigraphy results. Clinical and Experimental Metastasis. 2003;20:171. - PubMed
-
- Wymenga LF, Groenier K, Schuurman J, Boomsma JH, Elferink RO, Mensink HJ. Pretreatment levels of urinary deoxypyridinoline as a potential marker in patients with prostate cancer with or without bone metastasis. BJU International. 2001;88:231. - PubMed
-
- Plebani M, Bernardi D, Zaninotto M, De Paoli M, Secchiero S, Sciacovelli L. New and traditional serum markers of bone metabolism in the detection of skeletal metastases. Clinical Biochemistry. 1996;29:67. - PubMed
-
- Berruti A, Dogliotti L, Gorzegno G, Torta M, Tampellini M, Tucci M, et al. Differential patterns of bone turnover in relation to bone pain and disease extent in bone in cancer patients with skeletal metastases. Clinical Chemistry. 1999;45:1240. see comment. - PubMed
-
- Clarke NW, McClure J, George NJ. Morphometric evidence for bone resorption and replacement in prostate cancer. British Journal of Urology. 1991;68:74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
