

Economic evaluation of human papillomavirus vaccination in the United Kingdom
- PMID: 18640957
- PMCID: PMC2500202
- DOI: 10.1136/bmj.a769
Economic evaluation of human papillomavirus vaccination in the United Kingdom
Abstract
Objective: To assess the cost effectiveness of routine vaccination of 12 year old schoolgirls against human papillomavirus infection in the United Kingdom.
Design: Economic evaluation.
Setting: UK. Population Schoolgirls aged 12 or older.
Main outcome measures: Costs, quality adjusted life years (QALYs), and incremental cost effectiveness ratios for a range of vaccination options.
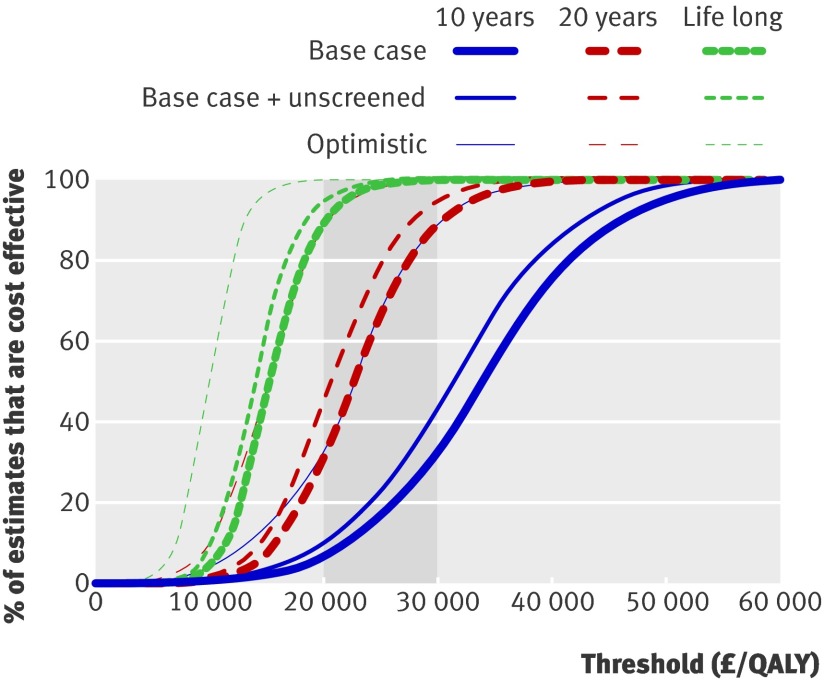
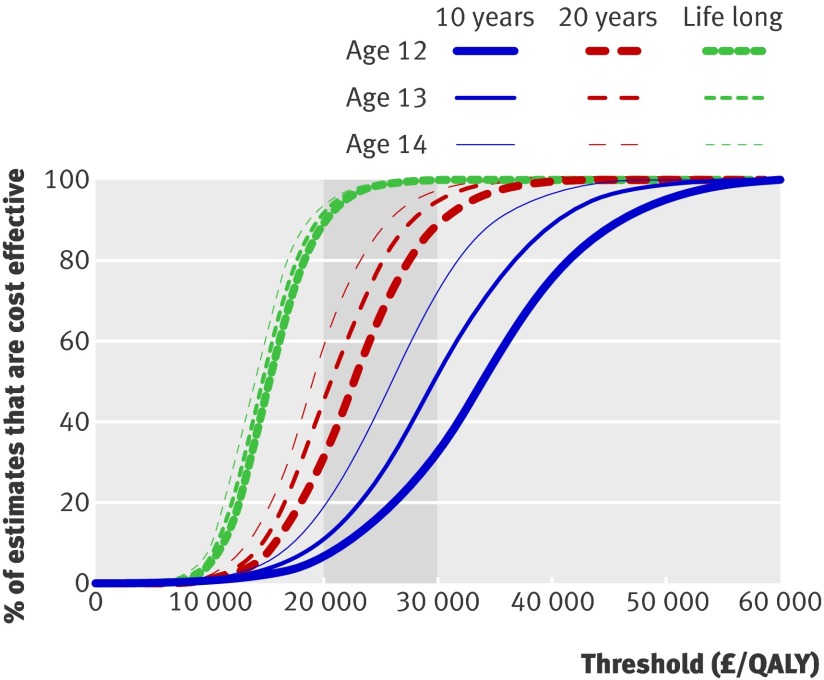
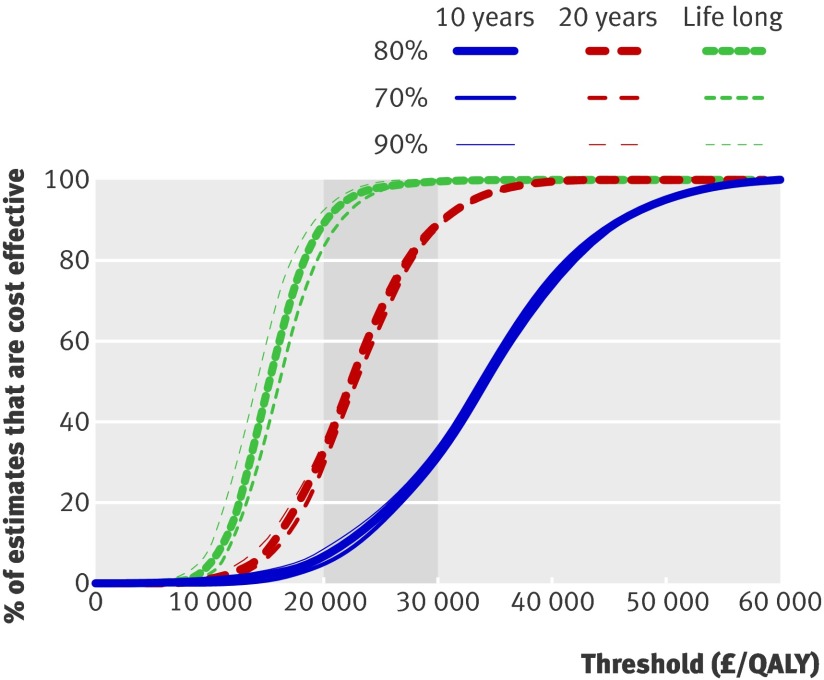
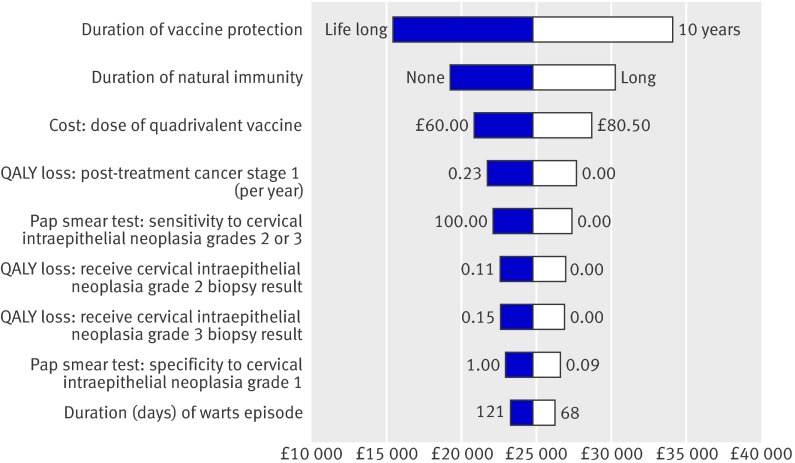
Results: Vaccinating 12 year old schoolgirls with a quadrivalent vaccine at 80% coverage is likely to be cost effective at a willingness to pay threshold of pound30,000 (euro37,700; $59,163) per QALY gained, if the average duration of protection from the vaccine is more than 10 years. Implementing a catch-up campaign of girls up to age 18 is likely to be cost effective. Vaccination of boys is unlikely to be cost effective. A bivalent vaccine with the same efficacy against human papillomavirus types 16 and 18 costing pound13- pound21 less per dose (depending on the duration of vaccine protection) may be as cost effective as the quadrivalent vaccine although less effective as it does not prevent anogenital warts.
Conclusions: Routine vaccination of 12 year old schoolgirls combined with an initial catch-up campaign up to age 18 is likely to be cost effective in the UK. The results are robust to uncertainty in many parameters and processes. A key influential variable is the duration of vaccine protection.
Conflict of interest statement
Competing interests: WJE’s partner works for GlaxoSmithKline.
Figures
Comment in
-
Human papillomavirus vaccination in the UK.BMJ. 2008 Jul 17;337:a842. doi: 10.1136/bmj.a842. BMJ. 2008. PMID: 18640958 No abstract available.
References
-
- Office for National Statistics. Cancer statistics 2004: registrations series MB1No 35. London: Office for National Statistics. 2008. www.statistics.gov.uk/statbase/Product.asp?vlnk=8843&More=N..
-
- Health Protection Agency. Trends in anogenital warts and anogenital herpes simplex virus infection in the United Kingdom: 1996 to 2005. CDR Weekly 2006;16.
-
- Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, Shah KV, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med 2003;348:518-27. - PubMed
-
- Von Krogh G, Lacey CJ, Gross G, Barrasso R, Schneider A. European guideline for the management of anogenital warts. Int J STD AIDS 2001;12(Suppl 3):40-7. - PubMed
-
- Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer 2006;118:3030-44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical