

Advantages of the nested case-control design in diagnostic research
- PMID: 18644127
- PMCID: PMC2500041
- DOI: 10.1186/1471-2288-8-48
Advantages of the nested case-control design in diagnostic research
Abstract
Background: Despite its benefits, it is uncommon to apply the nested case-control design in diagnostic research. We aim to show advantages of this design for diagnostic accuracy studies.
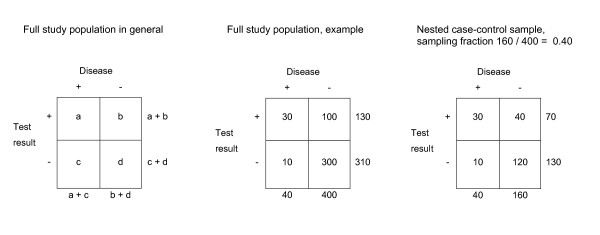
Methods: We used data from a full cross-sectional diagnostic study comprising a cohort of 1295 consecutive patients who were selected on their suspicion of having deep vein thrombosis (DVT). We draw nested case-control samples from the full study population with case:control ratios of 1:1, 1:2, 1:3 and 1:4 (per ratio 100 samples were taken). We calculated diagnostic accuracy estimates for two tests that are used to detect DVT in clinical practice.
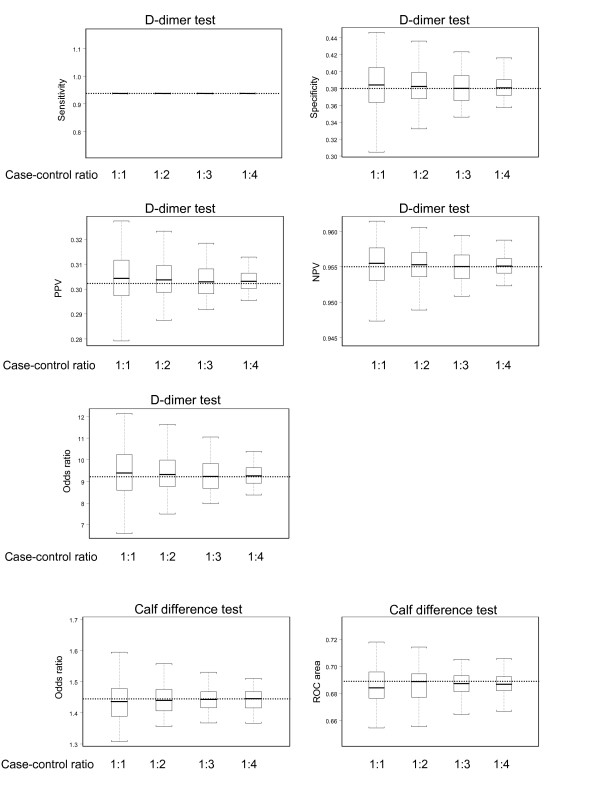
Results: Estimates of diagnostic accuracy in the nested case-control samples were very similar to those in the full study population. For example, for each case:control ratio, the positive predictive value of the D-dimer test was 0.30 in the full study population and 0.30 in the nested case-control samples (median of the 100 samples). As expected, variability of the estimates decreased with increasing sample size.
Conclusion: Our findings support the view that the nested case-control study is a valid and efficient design for diagnostic studies and should also be (re)appraised in current guidelines on diagnostic accuracy research.
Figures
References
-
- Whiting P, Rutjes AW, Reitsma JB, Glas AS, Bossuyt PM, Kleijnen J. Sources of variation and bias in studies of diagnostic accuracy: a systematic review. Ann Intern Med. 2004;140:189–202. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
