

Effect of increased pigmentation on the antifibrotic response of human skin to UV-A1 phototherapy
- PMID: 18645136
- PMCID: PMC2956589
- DOI: 10.1001/archderm.144.7.851
Effect of increased pigmentation on the antifibrotic response of human skin to UV-A1 phototherapy
Abstract
Objective: To investigate the efficacy, potential limitations, and biological mechanisms of UV-A1 phototherapy for skin sclerosis due to collagen deposition disorders.
Design: Before-and-after trial of UV-A1 irradiation of sclerotic skin; in vivo biochemical analyses after UV-A1 irradiation of normal skin.
Setting: Academic referral center.
Participants: Patients with morphea/scleroderma or sclerodermoid graft-vs-host disease and volunteers without skin disease. Intervention Sclerotic skin was treated with high-dose (130 J/cm(2); n = 12) or medium-dose (65 J/cm(2); n = 6) UV-A1 phototherapy 3 times per week for 14 weeks; normal skin was treated with UV-A1 irradiation at various doses and frequencies, with biopsies performed afterwards.
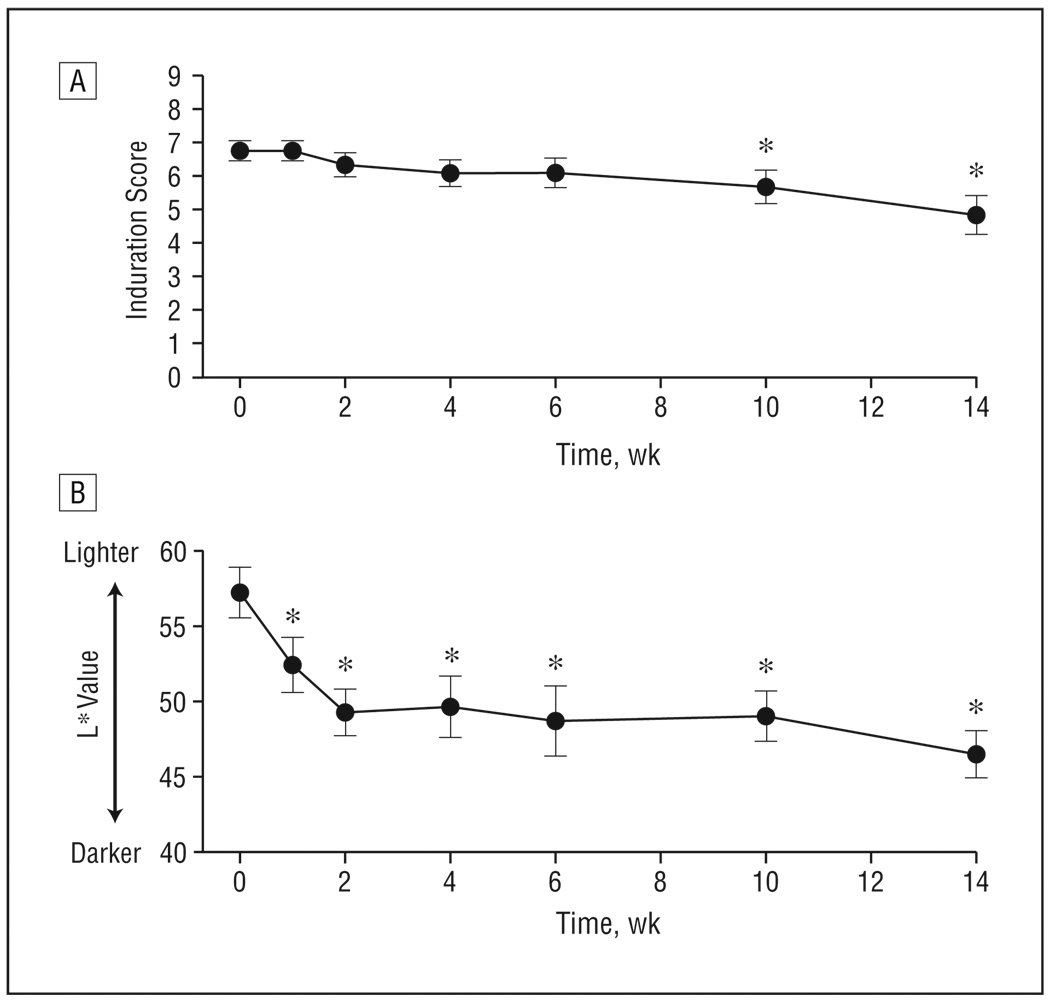
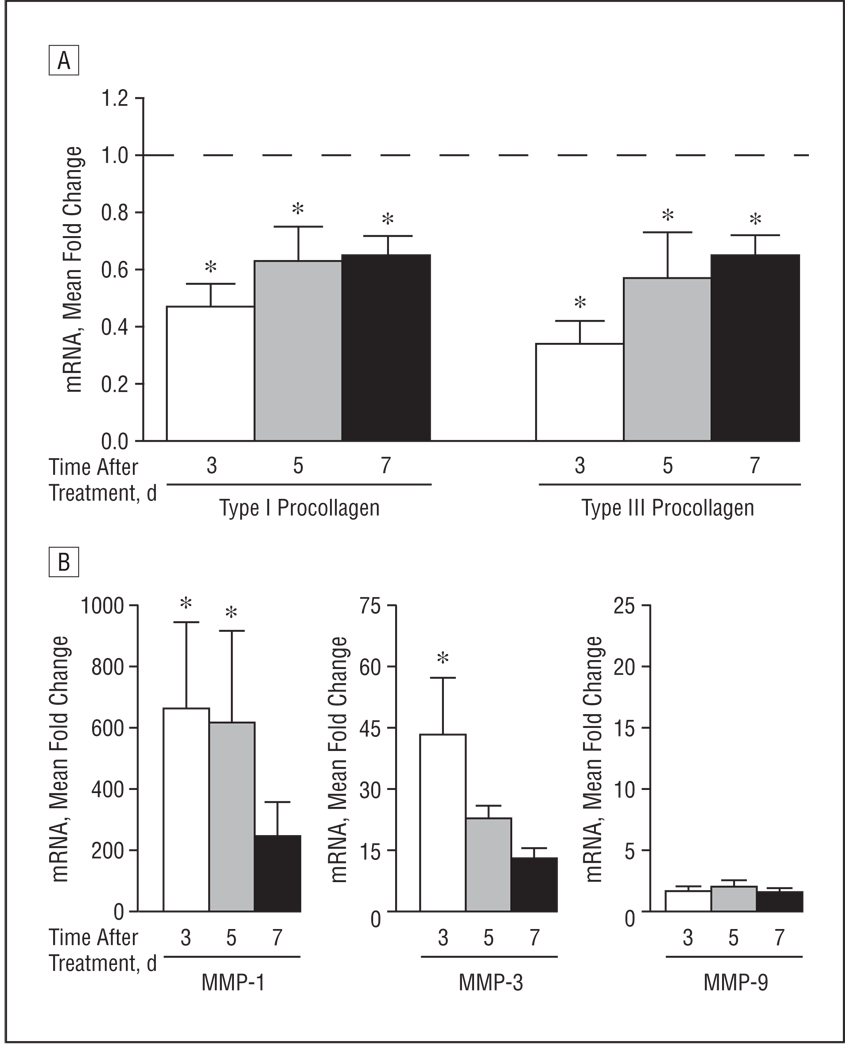
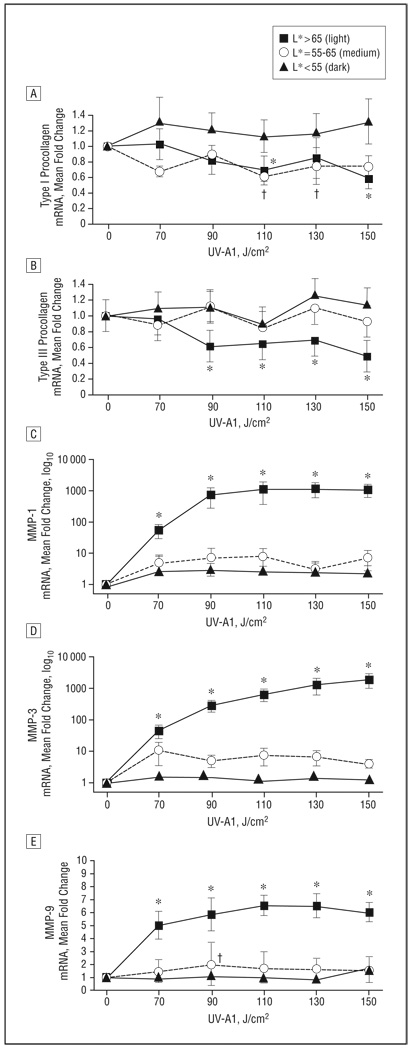
Main outcome measures: In sclerotic skin, induration was clinically assessed using a scoring scale. In normal skin, quantitative polymerase chain reaction was used to assess antifibrotic responses, defined as decreased type I and type III procollagen and increased matrix metalloproteinase levels.
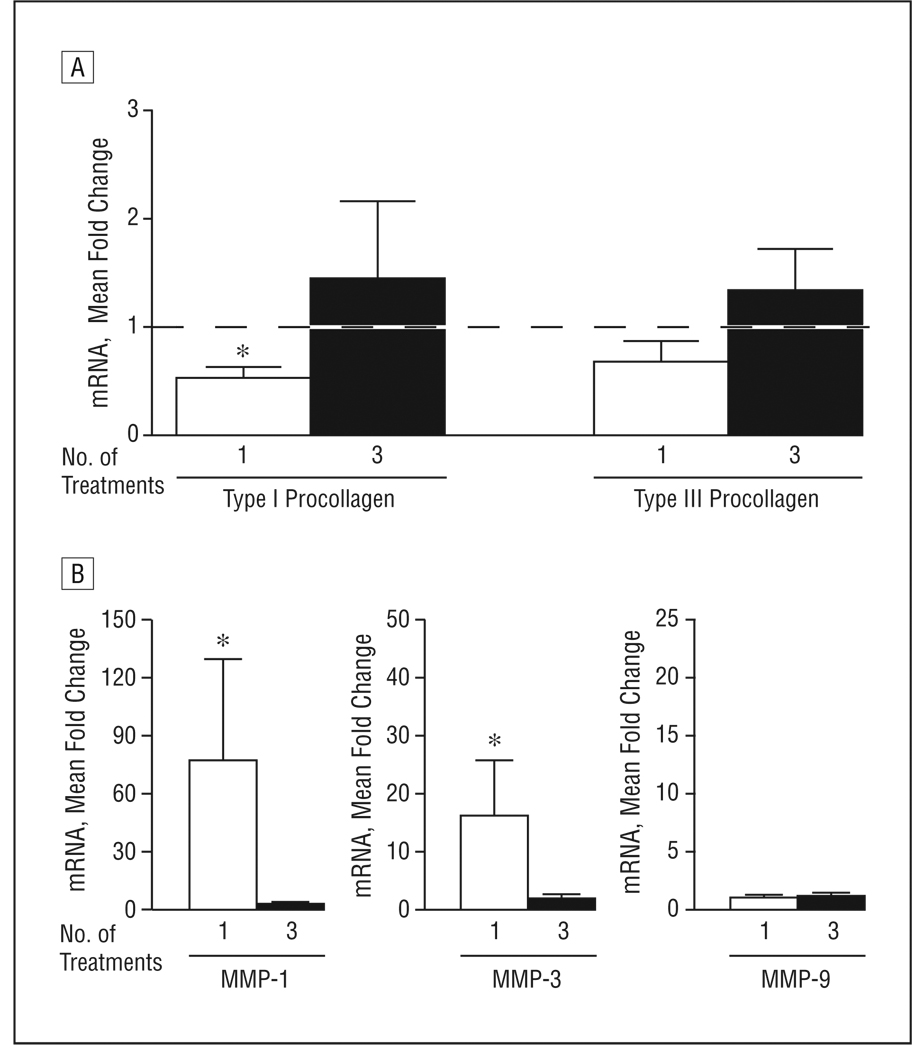
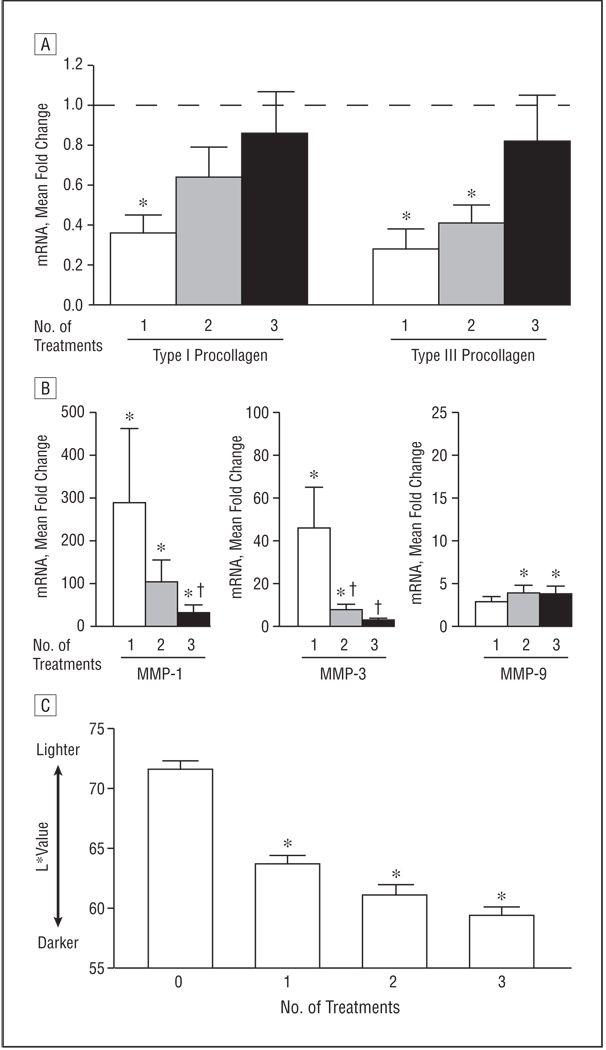
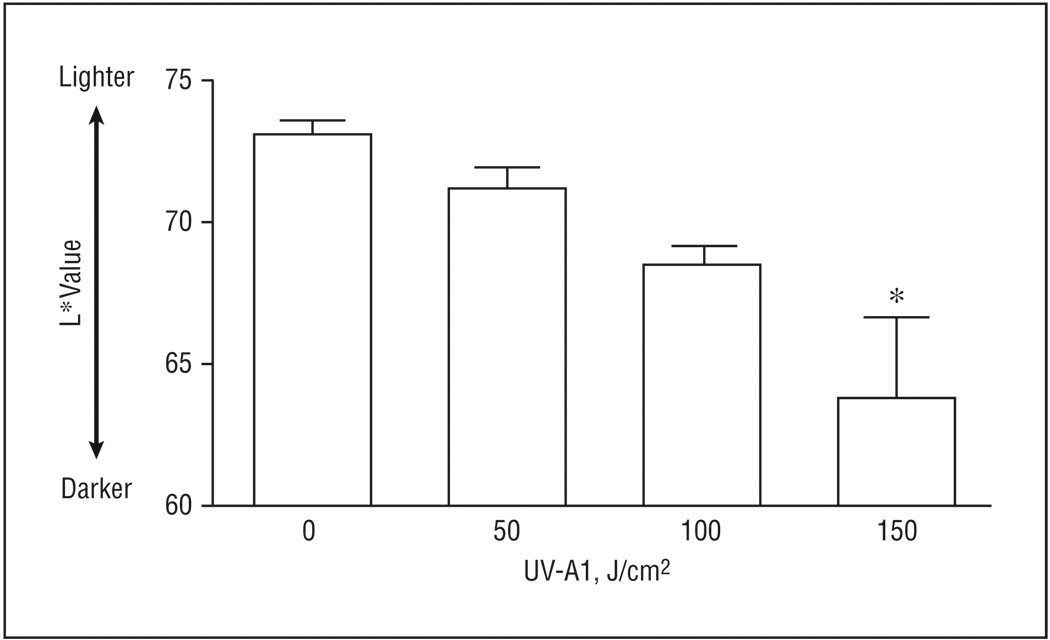
Results: In patients with sclerotic skin treated with high-dose UV-A1 irradiation, clinical scores for induration modestly decreased. To investigate what factors prevented further improvement (ie, complete clearance), normal skin with light pigmentation was exposed to UV-A1 irradiation (70-150 J/cm(2)) and was assessed for antifibrotic responses. A single high-dose exposure (110-150 J/cm(2)) elicited substantial antifibrotic responses and induced skin darkening. This skin darkening attenuated responses to subsequent UV-A1 exposures and was dose dependent. Thus, to minimize skin darkening, additional patients with sclerotic skin were treated with medium-dose UV-A1 phototherapy, which was no less effective than high-dose therapy.
Conclusion: Clinical responses of sclerotic skin to UV-A1 phototherapy were modest because of UV-A1-induced skin darkening, which is photoprotective and attenuates antifibrotic responses.
Trial registration: clinicaltrials.gov Identifier: NCT00129415.
Figures
Comment in
-
UV-A1 phototherapy for sclerotic skin diseases: implications for optimizing patient selection and management.Arch Dermatol. 2008 Jul;144(7):912-6. doi: 10.1001/archderm.144.7.912. Arch Dermatol. 2008. PMID: 18645143 No abstract available.
References
-
- Charles C, Clements P, Furst DE. Systemic sclerosis: hypothesis-driven treatment strategies. Lancet. 2006;367(9523):1683–1691. - PubMed
-
- Denton CP, Black CM. Targeted therapy comes of age in scleroderma. Trends Immunol. 2005;26(11):596–602. - PubMed
-
- Fisher GJ, Kang S. Phototherapy for scleroderma: biologic rationale, results, and promise. Curr Opin Rheumatol. 2002;14(6):723–726. - PubMed
-
- Denton CP, Black CM, Abraham DJ. Mechanisms and consequences of fibrosis in systemic sclerosis. Nat Clin Pract Rheumatol. 2006;2(3):134–144. - PubMed
