

Metabolic syndrome as a cardiovascular disease risk factor: patients evaluated in primary care
- PMID: 18647383
- PMCID: PMC2515316
- DOI: 10.1186/1471-2458-8-251
Metabolic syndrome as a cardiovascular disease risk factor: patients evaluated in primary care
Abstract
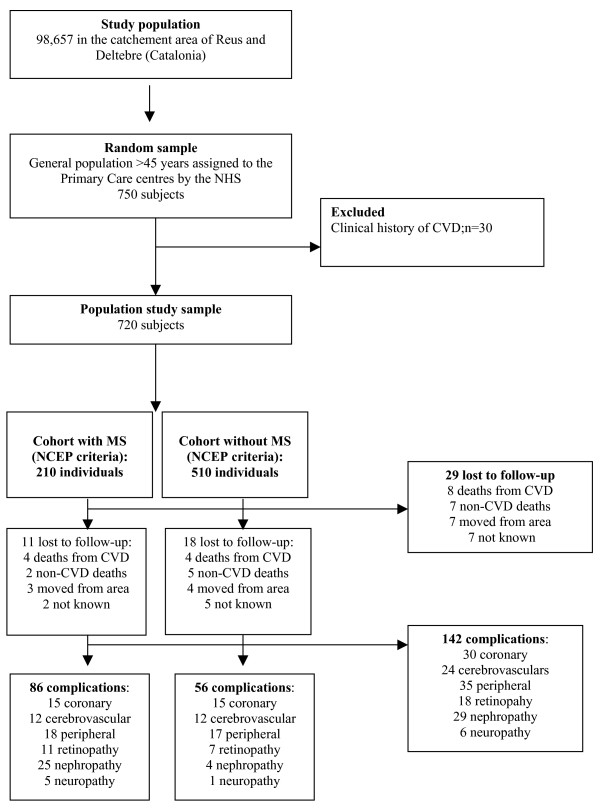
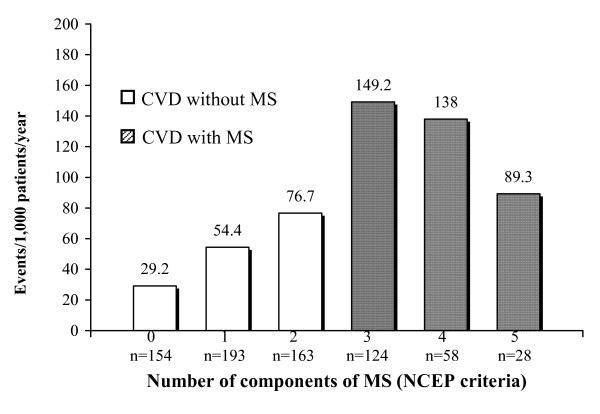
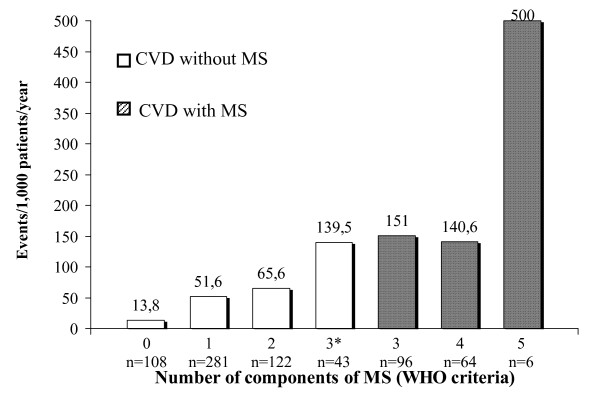
To estimate the prevalence of metabolic syndrome (MS) in a population receiving attention in primary care centers (PCC) we selected a random cohort of ostensibly normal subjects from the registers of 5 basic-health area (BHA) PCC. Diagnosis of MS was with the WHO, NCEP and IDF criteria. Variables recorded were: socio-demographic data, CVD risk factors including lipids, obesity, diabetes, blood pressure and smoking habit and a glucose tolerance test outcome. Of the 720 individuals selected (age 60.3 +/- 11.5 years), 431 were female, 352 hypertensive, 142 diabetic, 233 pre-diabetic, 285 obese, 209 dyslipemic and 106 smokers. CVD risk according to the Framingham and REGICOR calculation was 13.8 +/- 10% and 8.8 +/- 9.8%, respectively. Using the WHO, NCEP and IDF criteria, MS was diagnosed in 166, 210 and 252 subjects, respectively and the relative risk of CVD complications in MS subjects was 2.56. Logistic regression analysis indicated that the MS components (WHO set), the MS components (IDF set) and the female gender had an increased odds ratio for CVD of 3.48 (95CI%: 2.26-5.37), 2.28 (95%CI: 1.84-4.90) and 2.26 (95%CI: 1.48-3.47), respectively. We conclude that MS and concomitant CVD risk is high in ostensibly normal population attending primary care clinics, and this would necessarily impinge on resource allocation in primary care.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
