

Cytomegalovirus reactivation in critically ill immunocompetent patients
- PMID: 18647984
- PMCID: PMC2774501
- DOI: 10.1001/jama.300.4.413
Cytomegalovirus reactivation in critically ill immunocompetent patients
Abstract
Context: Cytomegalovirus (CMV) infection is associated with adverse clinical outcomes in immunosuppressed persons, but the incidence and association of CMV reactivation with adverse outcomes in critically ill persons lacking evidence of immunosuppression have not been well defined.
Objective: To determine the association of CMV reactivation with intensive care unit (ICU) and hospital length of stay in critically ill immunocompetent persons.
Design, setting, and participants: We prospectively assessed CMV plasma DNAemia by thrice-weekly real-time polymerase chain reaction (PCR) and clinical outcomes in a cohort of 120 CMV-seropositive, immunocompetent adults admitted to 1 of 6 ICUs at 2 separate hospitals at a large US tertiary care academic medical center between 2004 and 2006. Clinical measurements were assessed by personnel blinded to CMV PCR results. Risk factors for CMV reactivation and association with hospital and ICU length of stay were assessed by multivariable logistic regression and proportional odds models.
Main outcome measures: Association of CMV reactivation with prolonged hospital length of stay or death.
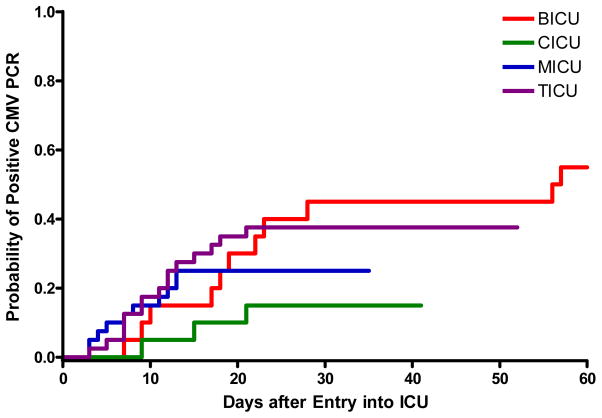
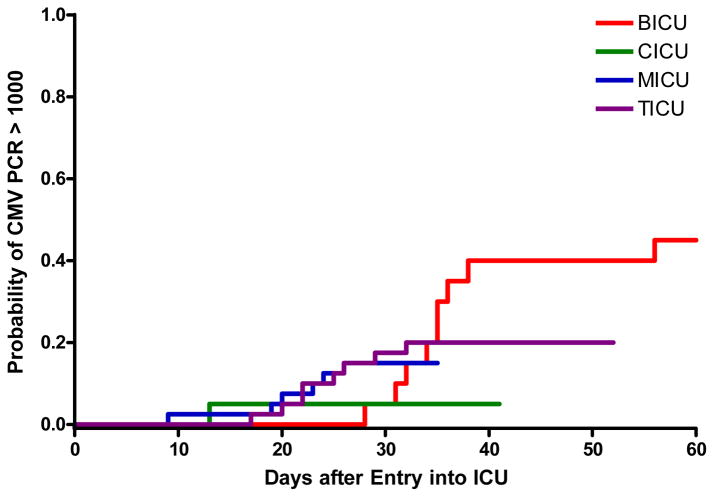
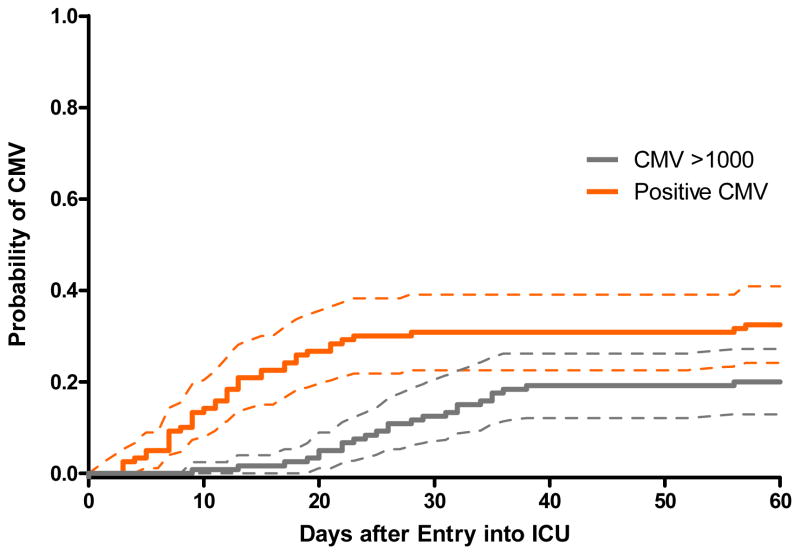
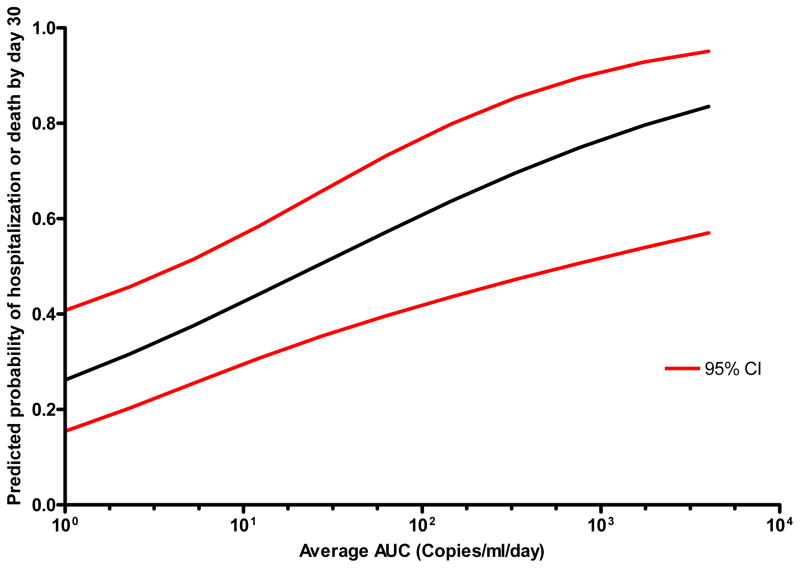
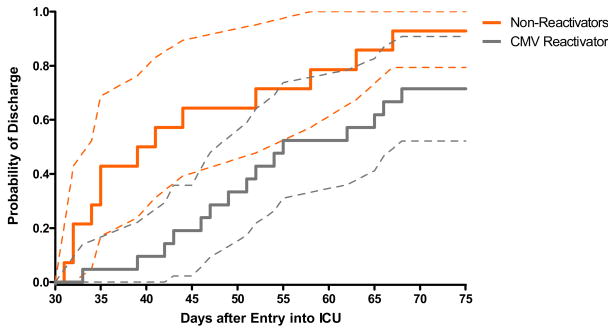
Results: The primary composite end point of continued hospitalization (n = 35) or death (n = 10) by 30 days occurred in 45 (35%) of the 120 patients. Cytomegalovirus viremia at any level occurred in 33% (39/120; 95% confidence interval [CI], 24%-41%) at a median of 12 days (range, 3-57 days) and CMV viremia greater than 1000 copies/mL occurred in 20% (24/120; 95% CI, 13%-28%) at a median of 26 days (range, 9-56 days). By logistic regression, CMV infection at any level (adjusted odds ratio [OR], 4.3; 95% CI, 1.6-11.9; P = .005) and at greater than 1000 copies/mL (adjusted OR, 13.9; 95% CI, 3.2-60; P < .001) and the average CMV area under the curve (AUC) in log(10) copies per milliliter (adjusted OR, 2.1; 95% CI, 1.3-3.2; P < .001) were independently associated with hospitalization or death by 30 days. In multivariable partial proportional odds models, both CMV 7-day moving average (OR, 5.1; 95% CI, 2.9-9.1; P < .001) and CMV AUC (OR, 3.2; 95% CI, 2.1-4.7; P < .001) were independently associated with a hospital length of stay of at least 14 days.
Conclusions: These preliminary findings suggest that reactivation of CMV occurs frequently in critically ill immunocompetent patients and is associated with prolonged hospitalization or death. A controlled trial of CMV prophylaxis in this setting is warranted.
Figures
Comment in
-
Reactivation of cytomegalovirus infection in critically ill immunocompetent patients.JAMA. 2008 Nov 26;300(20):2367-8; author reply 2368. doi: 10.1001/jama.2008.696. JAMA. 2008. PMID: 19033584 No abstract available.
References
-
- George MJ, Snydman DR, Werner BG, et al. The independent role of cytomegalovirus as a risk factor for invasive fungal disease in orthotopic liver transplant recipients. Boston Center for Liver Transplantation CMVIG-Study Group. Cytogam, MedImmune, Inc. Gaithersburg, Maryland. Am J Med. 1997 Aug;103(2):106–113. - PubMed
-
- Hodson EM, Jones CA, Webster AC, et al. Antiviral medications to prevent cytomegalovirus disease and early death in recipients of solid-organ transplants: a systematic review of randomised controlled trials. Lancet. 2005 Jun 18–24;365(9477):2105–2115. - PubMed
-
- Kalil AC, Levitsky J, Lyden E, Stoner J, Freifeld AG. Meta-analysis: the efficacy of strategies to prevent organ disease by cytomegalovirus in solid organ transplant recipients. Ann Intern Med. 2005 Dec 20;143(12):870–880. - PubMed
-
- Small LN, Lau J, Snydman DR. Preventing post-organ transplantation cytomegalovirus disease with ganciclovir: a meta-analysis comparing prophylactic and preemptive therapies. Clin Infect Dis. 2006 Oct 1;43(7):869–880. - PubMed
-
- Strippoli GF, Hodson EM, Jones C, Craig JC. Preemptive treatment for cytomegalovirus viremia to prevent cytomegalovirus disease in solid organ transplant recipients. Transplantation. 2006 Jan 27;81(2):139–145. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
