

Robotic assistance for ultrasound-guided prostate brachytherapy
- PMID: 18650122
- PMCID: PMC4724791
- DOI: 10.1016/j.media.2008.06.002
Robotic assistance for ultrasound-guided prostate brachytherapy
Abstract
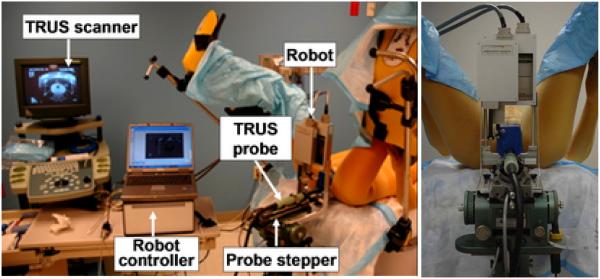
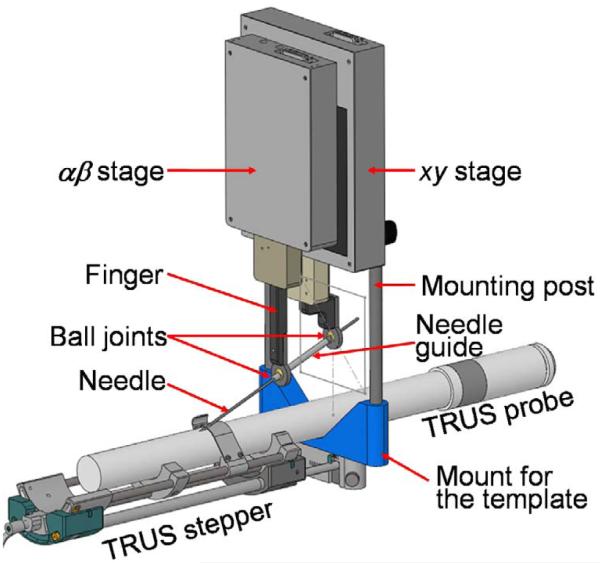
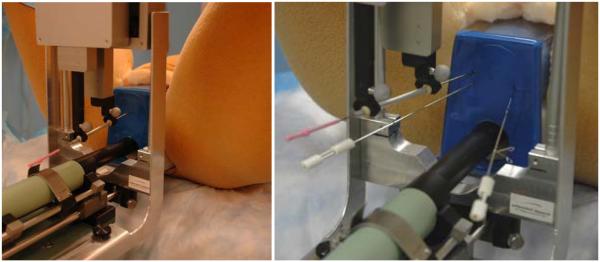
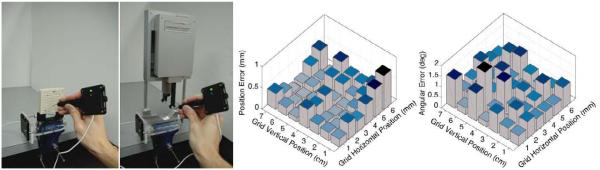
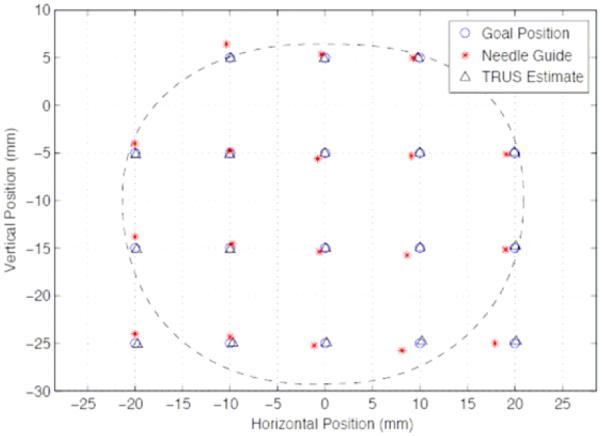
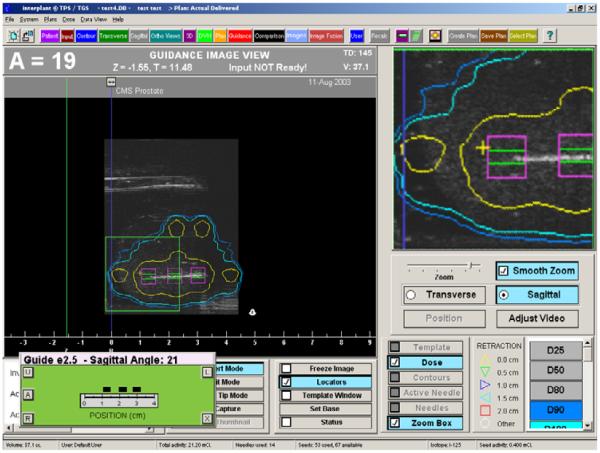
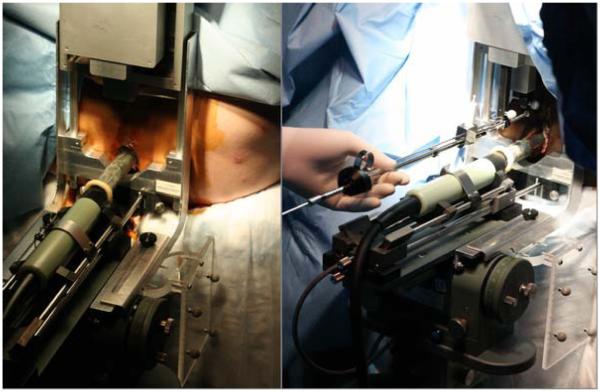
We present a robotically assisted prostate brachytherapy system and test results in training phantoms and Phase-I clinical trials. The system consists of a transrectal ultrasound (TRUS) and a spatially co-registered robot, fully integrated with an FDA-approved commercial treatment planning system. The salient feature of the system is a small parallel robot affixed to the mounting posts of the template. The robot replaces the template interchangeably, using the same coordinate system. Established clinical hardware, workflow and calibration remain intact. In all phantom experiments, we recorded the first insertion attempt without adjustment. All clinically relevant locations in the prostate were reached. Non-parallel needle trajectories were achieved. The pre-insertion transverse and rotational errors (measured with a Polaris optical tracker relative to the template's coordinate frame) were 0.25 mm (STD=0.17 mm) and 0.75 degrees (STD=0.37 degrees). In phantoms, needle tip placement errors measured in TRUS were 1.04 mm (STD=0.50mm). A Phase-I clinical feasibility and safety trial has been successfully completed with the system. We encountered needle tip positioning errors of a magnitude greater than 4mm in only 2 of 179 robotically guided needles, in contrast to manual template guidance where errors of this magnitude are much more common. Further clinical trials are necessary to determine whether the apparent benefits of the robotic assistant will lead to improvements in clinical efficacy and outcomes.
Figures

References
-
- Acher P, Popert R, Nichol J, Potters L, Morris S, Beaney R. Permanent prostate brachytherapy: Dosimetric results and analysis of a learning curve with a dynamic dose-feedback technique. Int J Radiat Oncol Biol Phys. 2006;65(3):694–698. - PubMed
-
- Alterovitz R, Goldberg K, Okamura A. Planning for Steerable Bevel-tip Needle Insertion Through 2D Soft Tissue with Obstacles. IEEE International Conference on Robotics and Automation (ICRA).2005. pp. 1652–1657.
-
- Brammer S, Merrick GS, Butler W, et al. The impact of needle trauma on urinary, bowel, and erectile function following transperineal template guided prostate saturation biopsy: implications for brachytherapy. Int J Radiat Oncol Biol Phys. 2007;69(Suppl.3):S350.
-
- Cooperberg MR, Broering JM, Litwin MS, et al. The contemporary management of prostate cancer in the United States: lessons from the cancer of the prostate strategic urologic research endeavor (CapSURE), a national disease registry. J Urol. 2004;171(4):1393–401. - PubMed
-
- DiMaio SP, Salcudean SE. Interactive simulation of needle insertion models. IEEE Trans Biomed Eng. 2005;52(7):1167–79. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
