

Aggressive immunosuppression minimization reduces graft loss following diagnosis of BK virus-associated nephropathy: a comparison of two reduction strategies
- PMID: 18650404
- PMCID: PMC2572268
- DOI: 10.2215/CJN.05691207
Aggressive immunosuppression minimization reduces graft loss following diagnosis of BK virus-associated nephropathy: a comparison of two reduction strategies
Abstract
Background and objectives: BK virus-associated nephropathy (BKVAN) has emerged as a leading cause of kidney graft loss, with no known predictors for graft loss and no consensus regarding treatment other than reduction of immunosuppression.
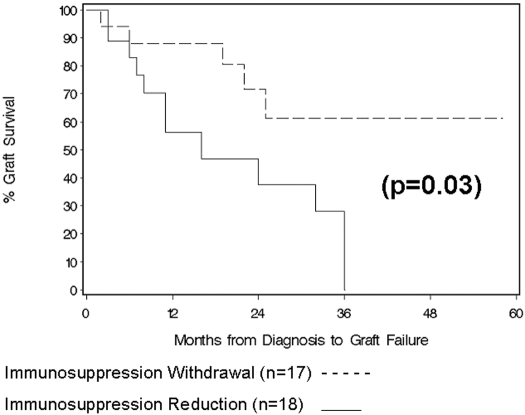
Design, setting, participants and measurements: A single-center retrospective analysis was performed of all cases of BKVAN from 1999 to 2005 for clinical predictors of graft loss, with evaluation of the impact of immunosuppression withdrawal (3-drug to 2-drug immunosuppression) within the first month versus reduction of immunosuppression.
Results: Of 910 kidney transplants, 35 (3.8%) cases of BKVAN were diagnosed at a median of 15 months after transplant (range, 5.5 to 90 months after transplant), 16 (46%) of which progressed to graft failure at a median of 11 months (range, 2 to 36 months) after diagnosis. Depleting antibody induction was a significant risk factor for graft loss on univariate analysis, whereas early drug withdrawal (<1 mo following diagnosis) protected against graft loss. On multivariate analysis, these findings were independent predictors of graft outcomes. Additionally, when patients were comanaged by referring nephrologists and the transplant center before the diagnosis of BKVAN, the risk of graft loss was 11-fold higher (P = 0.03) than if patients were managed solely by the transplant center.
Conclusions: Increased awareness and early diagnosis of BKVAN, with aggressive tapering of immunosuppression once established, is critical to preserve kidney graft function. Early drug withdrawal to low-dose two-drug therapy maintenance may be preferable to a general reduction of agents.
Figures

References
-
- Purighalla R, Shapiro R, McCauley J, Randhawa P: BK virus infection in a kidney allograft diagnosed by needle biopsy. Am J Kidney Dis 26: 671–673, 1995 - PubMed
-
- Mathur VS, Olson JL, Darragh TM, Yen TS: Polyomavirus-induced interstitial nephritis in two renal transplant recipients: case reports and review of the literature. Am J Kidney Dis 29: 754–758, 1997 - PubMed
-
- Randhawa PS, Finkelstein S, Scantlebury V, Shapiro R, Vivas C, Jordan M, Picken MM, Demetris AJ: Human polyoma virus-associated interstitial nephritis in the allograft kidney. Transplantation 67: 103–109, 1999 - PubMed
-
- Hirsch HH, Brennan DC, Drachenberg CB, Ginevri F, Gordon J, Limaye AP, Mihatsch MJ, Nickeleit V, Ramos E, Randhawa P, Shapiro R, Steiger J, Suthanthiran M, Trofe J: Polyomavirus-associated nephropathy in renal transplantation: interdisciplinary analyses and recommendations. Transplantation 79: 1277–1286, 2005 - PubMed
-
- Trofe J, Hirsch HH, Ramos E: Polyomavirus-associated nephropathy: update of clinical management in kidney transplant patients. Transpl Infect Dis 8: 76–85, 2006 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
