

Incidence and clinical characteristics of group A rotavirus infections among children admitted to hospital in Kilifi, Kenya
- PMID: 18651787
- PMCID: PMC2488191
- DOI: 10.1371/journal.pmed.0050153
Incidence and clinical characteristics of group A rotavirus infections among children admitted to hospital in Kilifi, Kenya
Abstract
Background: Rotavirus, predominantly of group A, is a major cause of severe diarrhoea worldwide, with the greatest burden falling on young children living in less-developed countries. Vaccines directed against this virus have shown promise in recent trials, and are undergoing effectiveness evaluation in sub-Saharan Africa. In this region limited childhood data are available on the incidence and clinical characteristics of severe group A rotavirus disease. Advocacy for vaccine intervention and interpretation of effectiveness following implementation will benefit from accurate base-line estimates of the incidence and severity of rotavirus paediatric admissions in relevant populations. The study objective was to accurately define the incidence and severity of group A rotavirus disease in a resource-poor setting necessary to make informed decisions on the need for vaccine prevention.
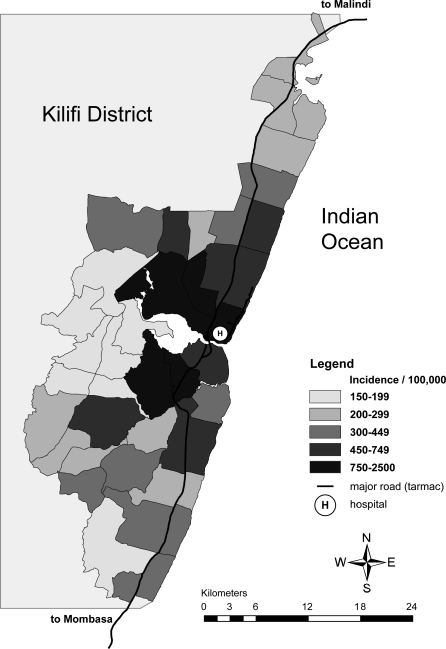
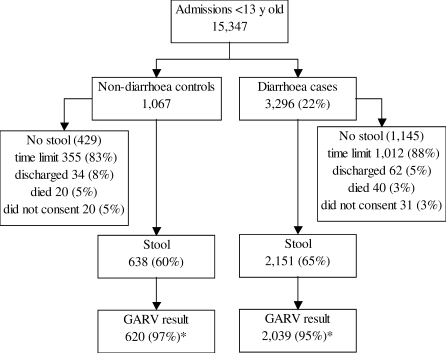
Methods and findings: Between 2002 and 2004 we conducted prospective surveillance for group A rotavirus infection at Kilifi District Hospital in coastal Kenya. Children < 13 y of age were eligible as "cases" if admitted with diarrhoea, and "controls" if admitted without diarrhoea. We calculated the incidence of hospital admission with group A rotavirus using data from a demographic surveillance study of 220,000 people in Kilifi District. Of 15,347 childhood admissions 3,296 (22%) had diarrhoea, 2,039 were tested for group A rotavirus antigen and, of these, 588 (29%) were positive. 372 (63%) rotavirus-positive cases were infants. Of 620 controls 19 (3.1%, 95% confidence interval [CI] 1.9-4.7) were rotavirus positive. The annual incidence (per 100,000 children) of rotavirus-positive admissions was 1,431 (95% CI 1,275-1,600) in infants and 478 (437-521) in under-5-y-olds, and highest proximal to the hospital. Compared to children with rotavirus-negative diarrhoea, rotavirus-positive cases were less likely to have coexisting illnesses and more likely to have acidosis (46% versus 17%) and severe electrolyte imbalance except hyponatraemia. In-hospital case fatality was 2% among rotavirus-positive and 9% among rotavirus-negative children.
Conclusions: In Kilifi > 2% of children are admitted to hospital with group A rotavirus diarrhoea in the first 5 y of life. This translates into over 28,000 vaccine-preventable hospitalisations per year across Kenya, and is likely to be a considerable underestimate. Group A rotavirus diarrhoea is associated with acute life-threatening metabolic derangement in otherwise healthy children. Although mortality is low in this clinical research setting this may not be generally true in African hospitals lacking rapid and appropriate management.
Conflict of interest statement
Figures
References
-
- Kapikian AZ, Hoshino Y, Chanock RM. Rotaviruses. In: Knipe DM, Howley PM, editors. Fields Virology. 4th ed. Philadelphia: Lippincott, Williams & Wilkins; 2001. pp. 1787–1833.
-
- Vesikari T, Matson DO, Dennehy P, Van Damme P, Santosham M, et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med. 2006;354:23–33. - PubMed
-
- Ruiz-Palacios GM, Perez-Schael I, Velazquez FR, Abate H, Breuer T, et al. Safety and efficacy of an attenuated vaccine against severe rotavirus gastroenteritis. N Engl J Med. 2006;354:11–22. - PubMed
