

Approaches to the diagnosis and grading of hiatal hernia
- PMID: 18656819
- PMCID: PMC2548324
- DOI: 10.1016/j.bpg.2007.12.007
Approaches to the diagnosis and grading of hiatal hernia
Abstract
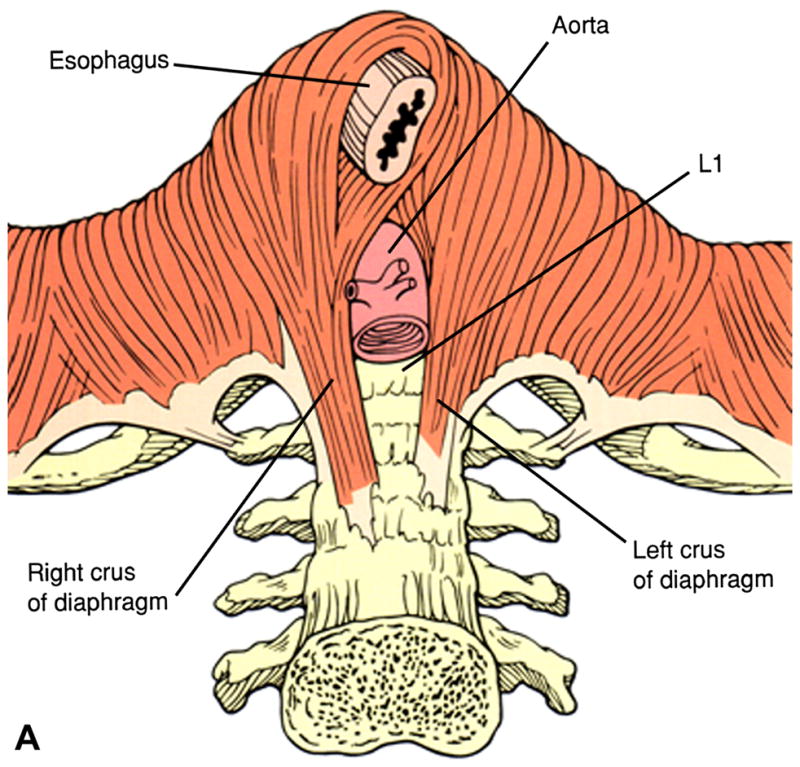
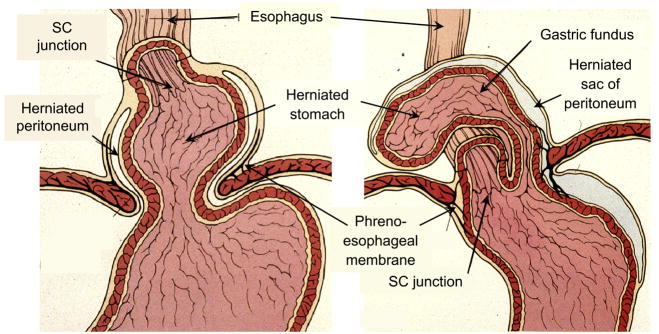
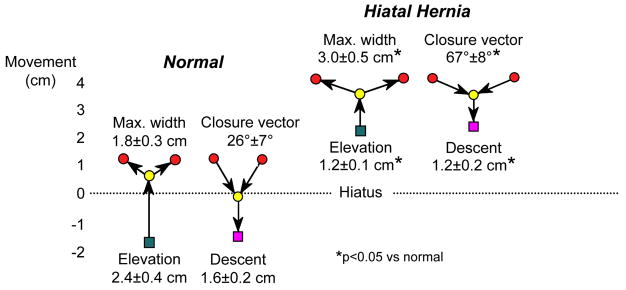
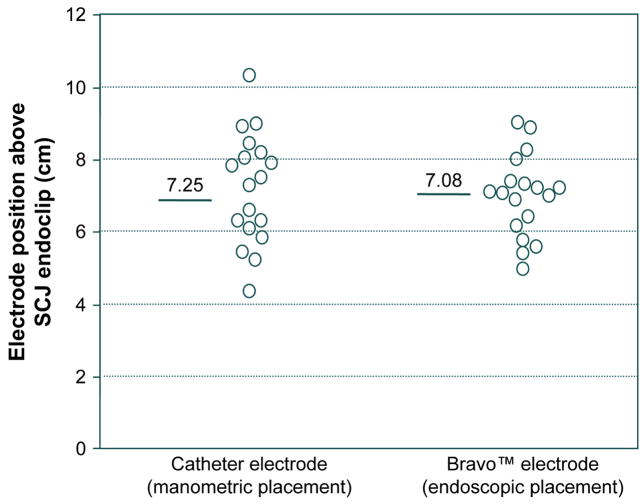
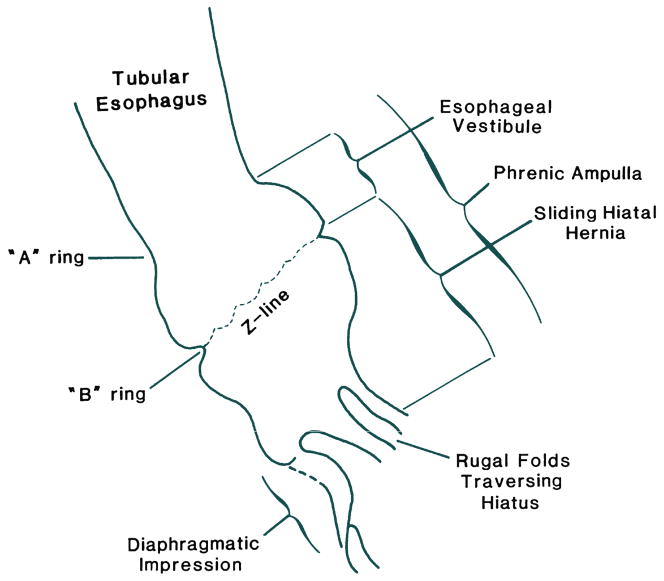
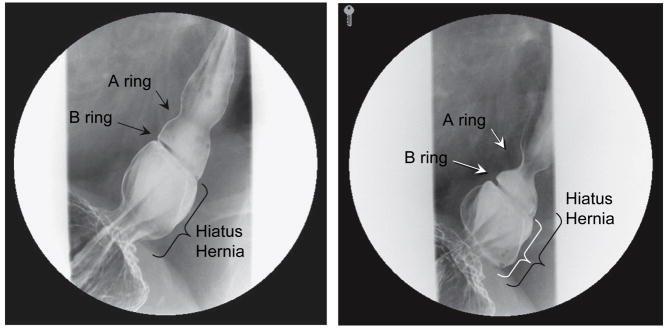
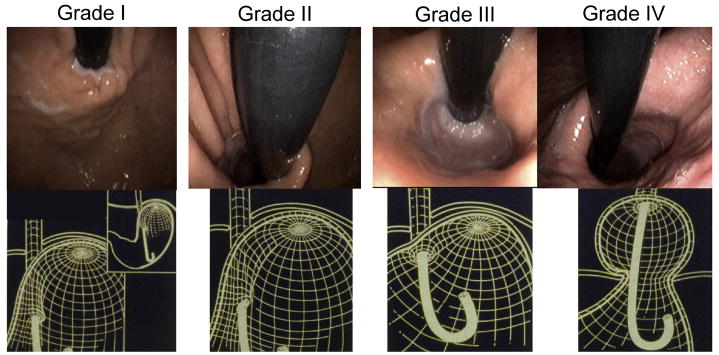
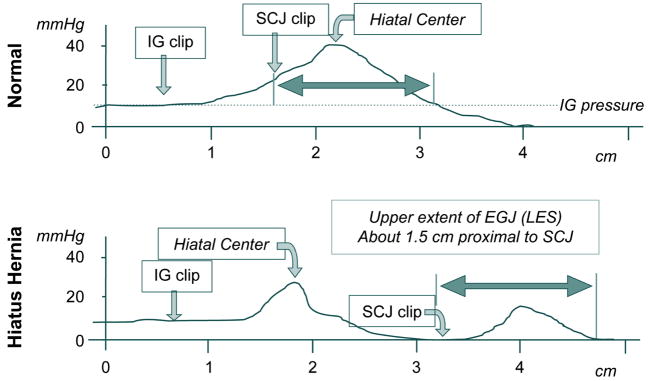
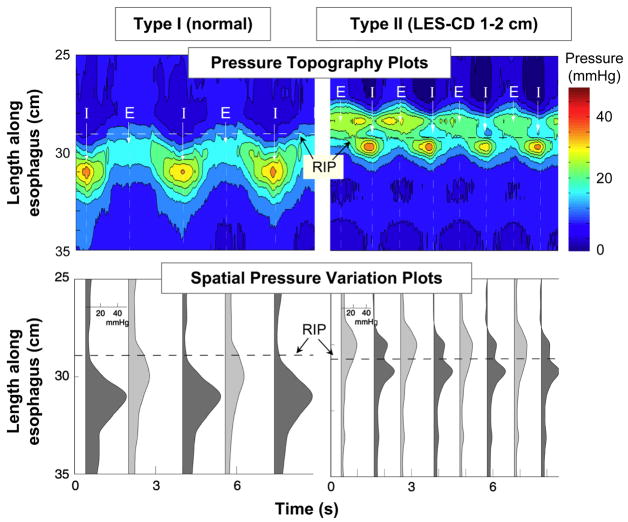
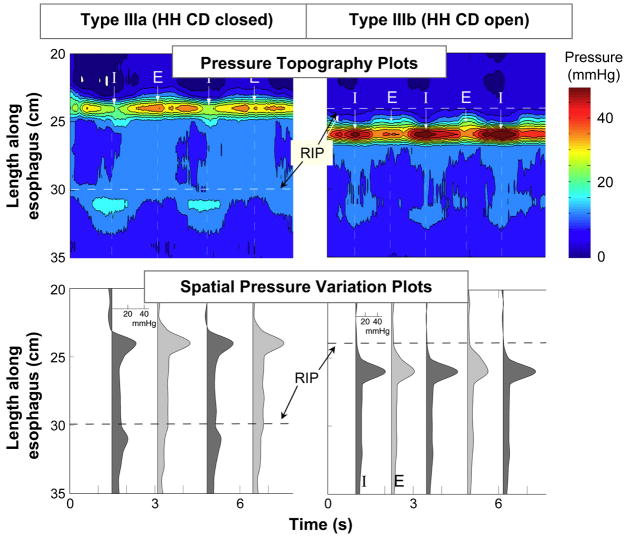
Hiatus hernia refers to conditions in which elements of the abdominal cavity, most commonly the stomach, herniate through the oesophageal hiatus into the mediastinum. With the most common type (type I or sliding hiatus hernia) this is associated with laxity of the phrenooesophageal membrane and the gastric cardia herniates. Sliding hiatus hernia is readily diagnosed by barium swallow radiography, endoscopy, or manometry when greater than 2 cm in axial span. However, the mobility of the oesophagogastric junction precludes the reliable detection of more subtle disruption by endoscopy or radiography. Detecting lesser degrees of axial separation between the lower oesophageal sphincter and crural diaphragm can only be reliably accomplished with high-resolution manometry, a technique that permits real time localization of these oesophagogastric junction components without swallow or distention related artefact.
Figures
References
-
- Marchand P. The anatomy of esophageal hiatus of the diaphragm and the pathogenesis of hiatus herniation. Thorac Surg. 1959;37:81–92. - PubMed
-
- Barrett NR. Discussion on hiatus hernia. Proc Roy Soc Med. 1932;122:736–796.
-
- Schatzki R. Die hernien des hiatus oesophageus. Deutsches Arch f klin med. 1932;173:85–103.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
