

Preoperative imaging of cervical pedicles: comparison of accuracy of oblique radiographs versus axial CT scans
- PMID: 18661159
- PMCID: PMC2527419
- DOI: 10.1007/s00586-008-0725-7
Preoperative imaging of cervical pedicles: comparison of accuracy of oblique radiographs versus axial CT scans
Abstract
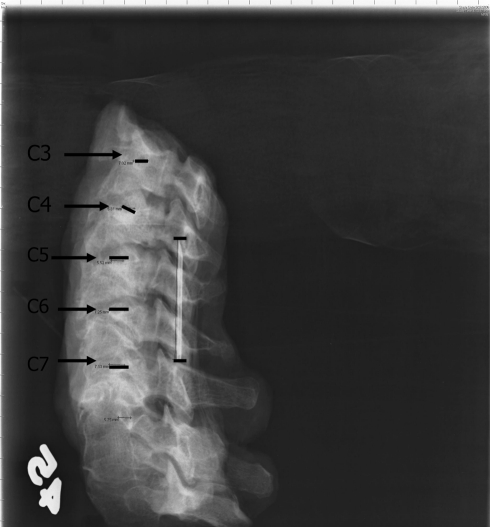
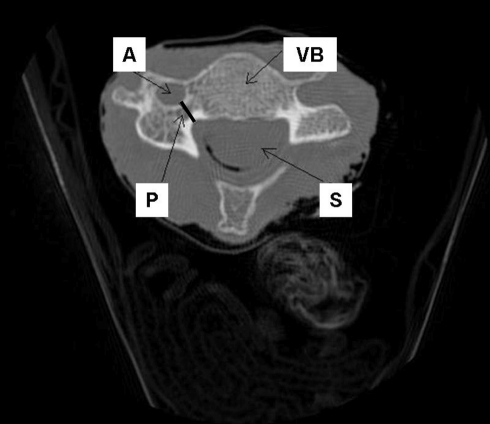
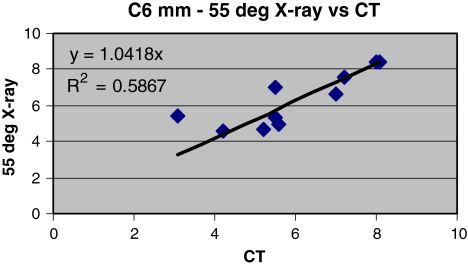
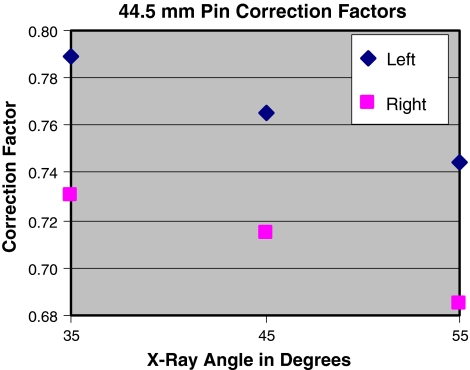
In spite of concerns about safety during their insertion, cervical spine pedicle screws have demonstrated biomechanical superiority over lateral mass screws in several biomechanical studies. One of the concerns for placement of cervical pedicle screws is their small size. Preoperative planning with computed tomography to assess pedicle width has been shown to be extremely accurate and is recommended by several authors. To date there has been no study assessing the accuracy of oblique radiographs for pedicle measurement. We sought to compare accuracy of the oblique radiographic measurements of cervical pedicle width with axial CT scan measurements. Five fresh-frozen human cadaveric cervical spines C3-C7 were studied. Thin cut 1.25 mm computed tomography axial cuts were made through the pedicle isthmus. Oblique radiographs at 35 degrees , 45 degrees , and 55 degrees angles were taken of the right and left pedicles of each specimen using a standardized technique. Each radiograph contained a pin of known length to correct for magnification. All pedicles were again measured and corrected for magnification using the standard pin. Corrected oblique radiograph measurements were compared to CT for each specimen. The outer pedicle width was measured and agreed upon by consensus. The radiograph measurements were on average significantly larger than CT measurements for the pedicles indicating that the pin standard did not completely correct magnification. Plain radiographic data failed to reveal that one oblique angle was favorable to another in terms of magnification or precision. Plain radiographs at oblique angles do not provide accurate measurements of subaxial cervical pedicles at 35 degrees , 45 degrees , or 55 degrees angles. We recommend that thin cut axial CT scans be obtained on all patients prior to transpedicular fixation in the cervical spine.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
