

doi: 10.2337/dc08-9021.
Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists
Affiliations
- PMID: 18663232
- PMCID: PMC2494620
- DOI: 10.2337/dc08-9021
Item in Clipboard
Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists
Diabetes Care.
2008 Aug.
No abstract available
Figures
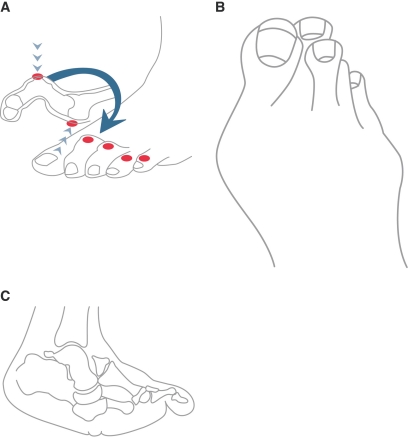
Foot deformities. These sites are frequent locations for diabetic foot ulceration. A: Claw toe deformity. Note the buckling phenomenon that causes increased pressure on the dorsal hammer digit deformity, as well as on the plantar metatarsal head. B: Bunion and overlapping toes. This deformity can lead to pressure ulceration between the digits, on the dorsal or plantar surfaces of displaced digits, and over the medial first metatarsophalangeal joint. C: A rocker-bottom deformity secondary to Charcot arthropathy can cause excessive pressure at the plantar midfoot, increasing risk for ulceration at that site.
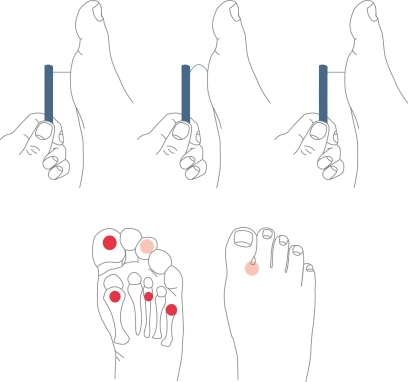
Upper panel: For performance of the 10-g monofilament test, the device is placed perpendicular to the skin, with pressure applied until the monofilament buckles. It should be held in place for ∼1 s and then released. Lower panel: The monofilament test should be performed at the highlighted sites while the patient's eyes are closed.
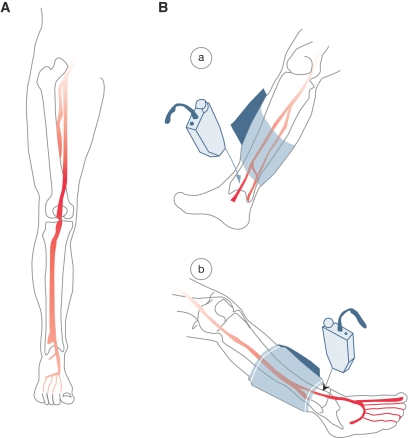
Lower-extremity circulation and the ABI test. A: Anterior view, right lower limb, normal arterial anatomy. B: ABI. Place blood pressure cuff above pulse. Place Doppler probe over arterial pulse; a: posterior tibial artery, b: dorsalis pedis artery. ABI calculation: Divide ankle systolic blood pressure by brachial artery systolic blood pressure. (ABI >0.9 is normal.) Adapted from Khan et al., JAMA 295:536–546, 2006.
Republished in
-
Comprehensive foot examination and risk assessment. A report of the Task Force of the Foot Care Interest Group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists.Phys Ther. 2008 Nov;88(11):1436-43. doi: 10.1093/ptj/88.11.1436. Phys Ther. 2008. PMID: 19137633 No abstract available.
References
-
- Mayfield JA, Reiber GE, Sanders LJ, Janisse D, Pogach LM: Preventive foot care in people with diabetes. Diabetes Care 21:2161–2177, 1998 - PubMed
-
- American Diabetes Association: Preventative foot care in people with diabetes. Diabetes Care 26(Suppl. 1):S78–S79, 2003 - PubMed
-
- Singh N, Armstrong DG, Lipsky BA: Preventing foot ulcers in patients with diabetes. JAMA 293:217–228, 2005 - PubMed
-
- Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW, Hussain A, Jackson N, Johnson KE, Ryder CH, Torkington R, Van Ross ER, Whalley AM, Widdows P, Williamson S, Boulton AJ: The North-West Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabet Med 19:377–384, 2002 - PubMed
-
- Reiber GE, Vileikyte L, Boyko EJ, del Aguila M, Smith DG, Lavery LA, Boulton AJ: Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care 22:157–162, 1999 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
