

Reliability of diagnostic coding in intensive care patients
- PMID: 18664267
- PMCID: PMC2575581
- DOI: 10.1186/cc6969
Reliability of diagnostic coding in intensive care patients
Abstract
Introduction: Administrative coding of medical diagnoses in intensive care unit (ICU) patients is mandatory in order to create databases for use in epidemiological and economic studies. We assessed the reliability of coding between different ICU physicians.
Method: One hundred medical records selected randomly from 29,393 cases collected between 1998 and 2004 in the French multicenter Outcomerea ICU database were studied. Each record was sent to two senior physicians from independent ICUs who recoded the diagnoses using the International Statistical Classification of Diseases and Related Health Problems: Tenth Revision (ICD-10) after being trained according to guidelines developed by two French national intensive care medicine societies: the French Society of Intensive Care Medicine (SRLF) and the French Society of Anesthesiology and Intensive Care Medicine (SFAR). These codes were then compared with the original codes, which had been selected by the physician treating the patient. A specific comparison was done for the diagnoses of septicemia and shock (codes derived from A41 and R57, respectively).
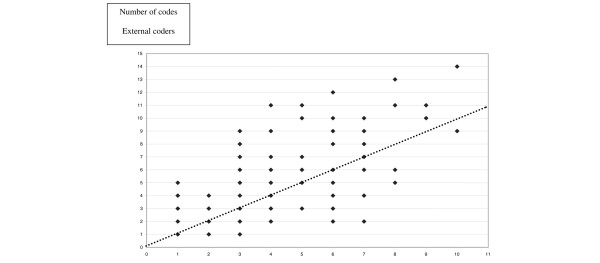
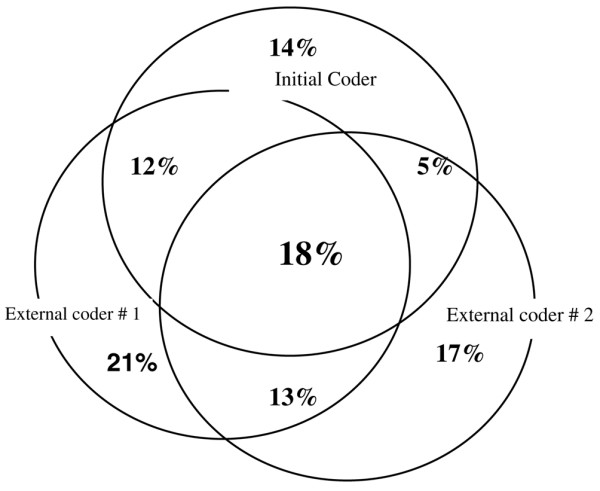
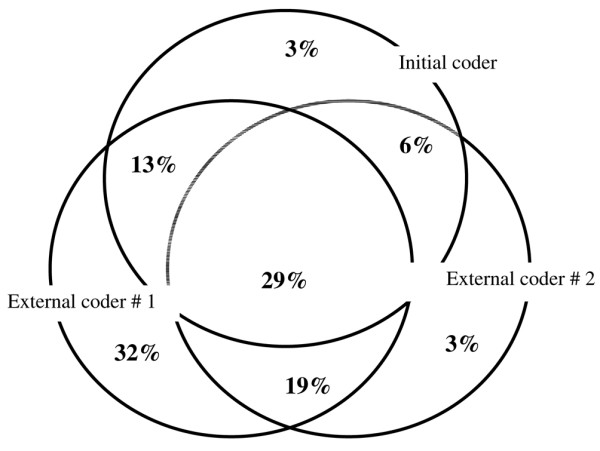
Results: The ICU physicians coded an average of 4.6 +/- 3.0 (range 1 to 32) diagnoses per patient, with little agreement between the three coders. The primary diagnosis was matched by both external coders in 34% (95% confidence interval (CI) 25% to 43%) of cases, by only one in 35% (95% CI 26% to 44%) of cases, and by neither in 31% (95% CI 22% to 40%) of cases. Only 18% (95% CI 16% to 20%) of all codes were selected by all three coders. Similar results were obtained for the diagnoses of septicemia and/or shock.
Conclusion: In a multicenter database designed primarily for epidemiological and cohort studies in ICU patients, the coding of medical diagnoses varied between different observers. This could limit the interpretation and validity of research and epidemiological programs using diagnoses as inclusion criteria.
Figures
Comment in
-
The essential nature of healthcare databases in critical care medicine.Crit Care. 2008;12(5):176. doi: 10.1186/cc6993. Epub 2008 Sep 1. Crit Care. 2008. PMID: 18771579 Free PMC article.
References
-
- Freeman JL, Fetter RB, Park H, Schneider KC, Lichtenstein JL, Hughes JS, Bauman WA, Duncan CC, Freeman DH, Jr, Palmer GR. Diagnosis-related group refinement with diagnosis- and procedure-specific comorbidities and complications. Med Care. 1995;33:806–827. doi: 10.1097/00005650-199508000-00006. - DOI - PubMed
-
- Holstein J, Taright N, Lepage E, Razafimamonjy J, Duboc D, Feldman L, Hittinger L, Lavergne T, Chatellier G. [Quality of medical database to valorize the DRG model by ISA cost indicators] Rev Epidemiol Sante Publique. 2002;50:593–603. - PubMed
-
- Timsit JF, Fosse JP, Troche G, De Lassence A, Alberti C, Garrouste-Orgeas M, Azoulay E, Chevret S, Moine P, Cohen Y. Accuracy of a composite score using daily SAPS II and LOD scores for predicting hospital mortality in ICU patients hospitalized for more than 72 h. Intensive Care Med. 2001;27:1012–1021. doi: 10.1007/s001340000840. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
