

Growth-differentiation factor-15 for early risk stratification in patients with acute chest pain
- PMID: 18664460
- PMCID: PMC2556729
- DOI: 10.1093/eurheartj/ehn339
Growth-differentiation factor-15 for early risk stratification in patients with acute chest pain
Abstract
Aims: Growth-differentiation factor-15 (GDF-15) has emerged as a biomarker of increased mortality and recurrent myocardial infarction (MI) in patients diagnosed with non-ST-elevation acute coronary syndrome. We explored the usefulness of GDF-15 for early risk stratification in 479 unselected patients with acute chest pain.
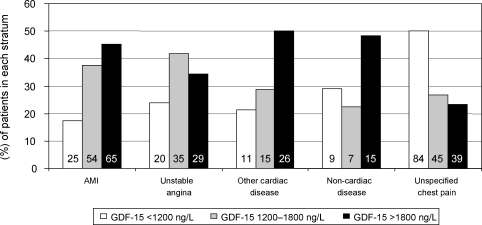
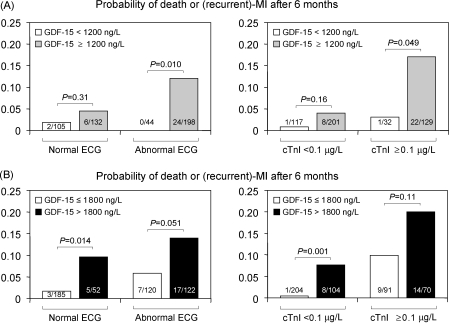
Methods and results: Sixty-nine per cent of the patients presented with GDF-15 levels above the previously defined upper reference limit (1200 ng/L). The risks of the composite endpoint of death or (recurrent) MI after 6 months were 1.3, 5.1, and 12.6% in patients with normal (<1200 ng/L), moderately elevated (1200-1800 ng/L), or markedly elevated (>1800 ng/L) levels of GDF-15 on admission, respectively (P < 0.001). By multivariable analysis that included clinical characteristics, ECG findings, peak cardiac troponin I levels within 2 h (cTnI(0-2 h)), N-terminal pro-B-type natriuretic peptide, C-reactive protein, and cystatin C, GDF-15 remained an independent predictor of the composite endpoint. The ability of the ECG combined with peak cTnI(0-2 h) to predict the composite endpoint was markedly improved by addition of GDF-15 (c-statistic, 0.74 vs. 0.83; P < 0.001).
Conclusion: GDF-15 improves risk stratification in unselected patients with acute chest pain and provides prognostic information beyond clinical characteristics, the ECG, and cTnI.
Figures

Comment in
-
Growth-differentiation factor-15 for risk stratification in patients with acute chest pain.Eur Heart J. 2008 Dec;29(23):2947; author reply 2947-8. doi: 10.1093/eurheartj/ehn457. Epub 2008 Oct 16. Eur Heart J. 2008. PMID: 18927212 No abstract available.
References
-
- Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A, Fernandez-Aviles F, Fox KA, Hasdai D, Ohman EM, Wallentin L, Wijns W, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Kristensen SD, Widimsky P, McGregor K, Sechtem U, Tendera M, Hellemans I, Gomez JL, Silber S, Funck-Brentano C, Andreotti F, Benzer W, Bertrand M, Betriu A, DeSutter J, Falk V, Ortiz AF, Gitt A, Hasin Y, Huber K, Kornowski R, Lopez-Sendon J, Morais J, Nordrehaug JE, Steg PG, Thygesen K, Tubaro M, Turpie AG, Verheugt F, Windecker S. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology. Eur Heart J. 2007;28:1598–1660. - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DEJ, Chavey WEn, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction): developed in collaboration with the American College of Emergency Physicians, American College of Physicians, Society for Academic Emergency Medicine, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2007;50:e1–e157. - PubMed
-
- Heeschen C, Goldmann BU, Langenbrink L, Matschuck G, Hamm CW. Evaluation of a rapid whole blood ELISA for quantification of troponin I in patients with acute chest pain. Clin Chem. 1999;45:1789–1796. - PubMed
-
- Jernberg T, Lindahl B. A combination of troponin T and 12-lead electrocardiography: a valuable tool for early prediction of long-term mortality in patients with chest pain without ST-segment elevation. Am Heart J. 2002;144:804–810. - PubMed
-
- Kontos MC, Shah R, Fritz LM, Anderson FP, Tatum JL, Ornato JP, Jesse RL. Implication of different cardiac troponin I levels for clinical outcomes and prognosis of acute chest pain patients. J Am Coll Cardiol. 2004;43:958–965. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
