

Correlates of low testosterone and symptomatic androgen deficiency in a population-based sample
- PMID: 18664536
- PMCID: PMC2579652
- DOI: 10.1210/jc.2008-0021
Correlates of low testosterone and symptomatic androgen deficiency in a population-based sample
Abstract
Context: Risk factors for low testosterone and symptomatic androgen deficiency (AD) may be modifiable.
Objective: Our objective was to examine demographic, anthropometric, and medical correlates of low testosterone and symptomatic AD.
Design: Data were used from the Boston Area Community Health Survey, an epidemiological study conducted from 2002-2005.
Setting: Data were obtained from a community-based random sample of racially and ethnically diverse men.
Patients or other participants: Data were available for 1822 men.
Main outcome measures: Multivariate logistic regression was used to estimate odds ratios (OR) and 95% confidence intervals (CI) for associations of covariates with 1) low testosterone and 2) symptomatic AD. The operational definition of low testosterone was serum total testosterone less than 300 ng/dl and free testosterone less than 5 ng/dl; symptomatic AD was defined as the additional presence of symptoms: any of low libido, erectile dysfunction, or osteoporosis or two or more of sleep disturbance, depressed mood, lethargy, or diminished physical performance.
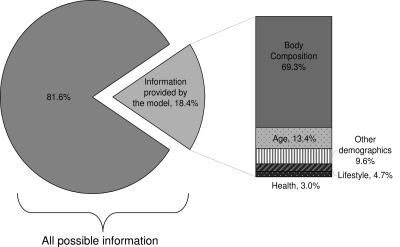
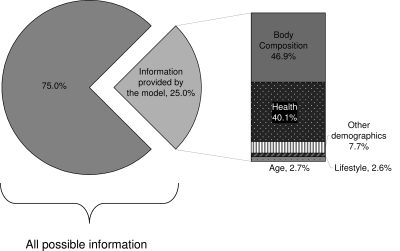
Results: Factors associated with low testosterone included age (OR = 1.36; 95% CI= 1.11-1.66, per decade), low per-capita income ($6000 or less per household member vs. more than $30,000; OR = 2.86; 95% CI = 1.39-5.87), and waist circumference (per 10-cm increase; OR = 1.75; 95% CI = 1.45-2.12). Only age (OR = 1.36; 95% CI = 1.04-1.77), waist circumference (OR = 1.88; 95% CI = 1.44-2.47), and health status (OR = 0.21; 95% CI = 0.05-0.92, excellent vs. fair/poor) were associated with our construct of symptomatic AD. Of all variables, waist circumference was the most important contributor in both models.
Conclusions: Waist circumference is a potentially modifiable risk factor for low testosterone and symptomatic AD. Manifestation of symptoms may be a consequence of generally poor health status.
Figures
Similar articles
-
Prevalence of symptomatic androgen deficiency in men.J Clin Endocrinol Metab. 2007 Nov;92(11):4241-7. doi: 10.1210/jc.2007-1245. Epub 2007 Aug 14. J Clin Endocrinol Metab. 2007. PMID: 17698901 Clinical Trial.
-
Treatment of symptomatic androgen deficiency: results from the Boston Area Community Health Survey.Arch Intern Med. 2008 May 26;168(10):1070-6. doi: 10.1001/archinte.168.10.1070. Arch Intern Med. 2008. PMID: 18504335
-
The prevalence of and risk factors for androgen deficiency in aging Taiwanese men.J Sex Med. 2009 Apr;6(4):936-946. doi: 10.1111/j.1743-6109.2008.01171.x. Epub 2008 Feb 9. J Sex Med. 2009. PMID: 19210712
-
[PADAM from the urologic viewpoint].Urologe A. 2000 Sep;39(5):407-10. doi: 10.1007/s001200050381. Urologe A. 2000. PMID: 11045038 Review. German.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Development of a men's Preference for Testosterone Replacement Therapy (P-TRT) instrument.Patient Prefer Adherence. 2012;6:631-41. doi: 10.2147/PPA.S35840. Epub 2012 Aug 31. Patient Prefer Adherence. 2012. PMID: 22969294 Free PMC article.
-
Cohort profile: the Boston Area Community Health (BACH) survey.Int J Epidemiol. 2014 Feb;43(1):42-51. doi: 10.1093/ije/dys198. Epub 2012 Dec 5. Int J Epidemiol. 2014. PMID: 23220718 Free PMC article.
-
Hormone replacement therapy and physical function in healthy older men. Time to talk hormones?Endocr Rev. 2012 Jun;33(3):314-77. doi: 10.1210/er.2012-1002. Epub 2012 Mar 20. Endocr Rev. 2012. PMID: 22433122 Free PMC article. Review.
-
The practical management of testosterone deficiency in men.Nat Rev Urol. 2015 Nov;12(11):641-50. doi: 10.1038/nrurol.2015.238. Epub 2015 Oct 13. Nat Rev Urol. 2015. PMID: 26458755 Review.
-
Relative contributions of multiple determinants to bone mineral density in men.Osteoporos Int. 2009 Dec;20(12):2035-47. doi: 10.1007/s00198-009-0895-0. Epub 2009 Mar 25. Osteoporos Int. 2009. PMID: 19319620 Free PMC article.
References
-
- US Department of Health and Human Services 2003 National Health and Nutrition Examination Survey data briefs: healthy weight, overweight, and obesity among U.S. adults. Atlanta, GA: Centers for Disease Control and Prevention
-
- Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM 2006 Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 91:1995–2010 - PubMed
-
- Kaufman JM, Vermeulen A 2005 The decline of androgen levels in elderly men and its clinical and therapeutic implications. Endocr Rev 26:833–876 - PubMed
-
- Wong SY, Chan DC, Hong A, Woo J 2006 Prevalence of and risk factors for androgen deficiency in middle-aged men in Hong Kong. Metabolism 55:1488–1494 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
