

Selecting high priority quality measures for breast cancer quality improvement
- PMID: 18665055
- PMCID: PMC3538153
- DOI: 10.1097/MLR.0b013e318178ead3
Selecting high priority quality measures for breast cancer quality improvement
Abstract
Background: Although many quality measures have been created, there is no consensus regarding which are the most important. We sought to develop a simple, explicit strategy for prioritizing breast cancer quality measures based on their potential to highlight areas where quality improvement efforts could most impact a population.
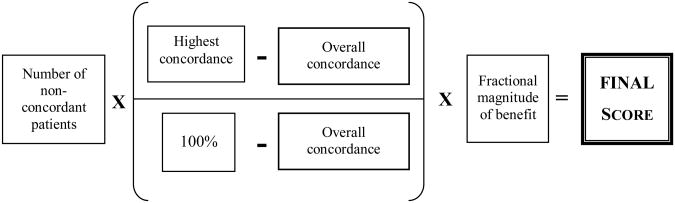
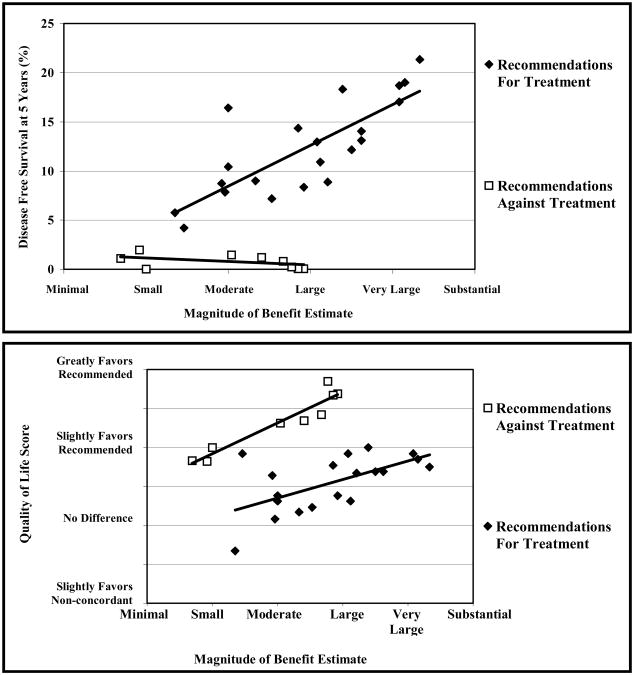
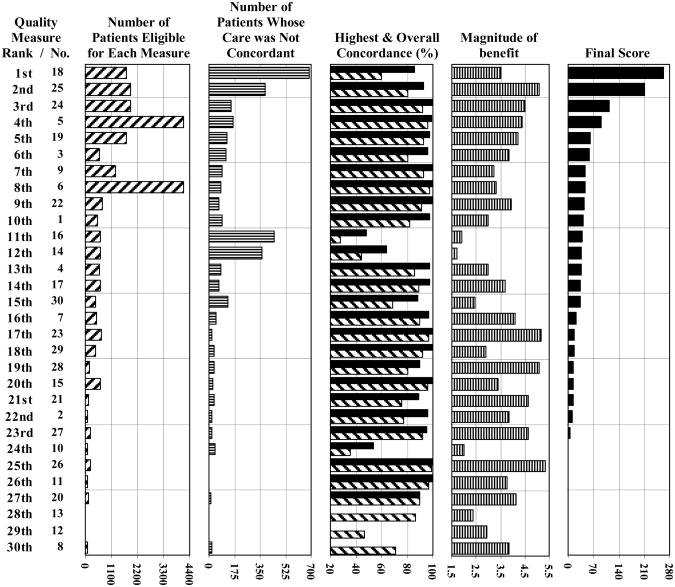
Methods: Using performance data for 9019 breast cancer patients treated at 10 National Comprehensive Cancer Network institutions, we assessed concordance relative to 30 reliable, valid breast cancer process-based treatment measures. We identified 4 attributes that indicated there was room for improvement and characterized the extent of burden imposed by failing to follow each measure: number of nonconcordant patients, concordance across all institutions, highest concordance at any 1 institution, and magnitude of benefit associated with concordant care. For each measure, we used data from the concordance analyses to derive the first 3 attributes and surveyed expert breast cancer physicians to estimate the fourth. A simple algorithm incorporated these attributes and produced a final score for each measure; these scores were used to rank the measures.
Results: We successfully prioritized quality measures using explicit, objective methods and actual performance data. The number of nonconcordant patients had the greatest influence on the rankings. The highest-ranking measures recommended chemotherapy and hormone therapy for hormone-receptor positive tumors and radiation therapy after breast-conserving surgery.
Conclusions: This simple, explicit approach is a significant departure from methods used previously, and effectively identifies breast cancer quality measures that have broad clinical relevance. Systematically prioritizing quality measures could increase the efficiency and efficacy of quality improvement efforts and substantially improve outcomes.
Figures
Comment in
-
On the road to improving the quality of breast cancer care: a distance still to travel.Med Care. 2008 Aug;46(8):759-61. doi: 10.1097/MLR.0b013e3181844867. Med Care. 2008. PMID: 18665054 No abstract available.
References
-
- Basch P. Quality of health care delivered to adults in the United States. New England Journal of Medicine. 2003;349:1866–8. comment. author reply 1866-8. - PubMed
-
- Kohn LT, Corrigan J, Donaldson MS. To err is human: building a safer health system. Washington, D.C.: National Academy Press; 2000. - PubMed
-
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. New England Journal of Medicine. 2003;348:2635–45. see comment. - PubMed
-
- Ray-Coquard I, Philip T, de Laroche G, et al. Persistence of medical change at implementation of clinical guidelines on medical practice: a controlled study in a cancer network. Journal of Clinical Oncology. 2005;23:4414–23. - PubMed
-
- Borenstein J, Badamgarav E, Henning JM, et al. The association between quality improvement activities performed by managed care organizations and quality of care. American Journal of Medicine. 2004;117:297–304. see comment. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
