

Not all missed doses are the same: sustained NNRTI treatment interruptions predict HIV rebound at low-to-moderate adherence levels
- PMID: 18665246
- PMCID: PMC2467488
- DOI: 10.1371/journal.pone.0002783
Not all missed doses are the same: sustained NNRTI treatment interruptions predict HIV rebound at low-to-moderate adherence levels
Abstract
Background: While the relationship between average adherence to HIV potent antiretroviral therapy is well defined, the relationship between patterns of adherence within adherence strata has not been investigated. We examined medication event monitoring system (MEMS) defined adherence patterns and their relation to subsequent virologic rebound.
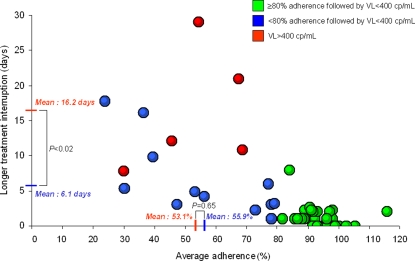
Methods and results: We selected subjects with at least 3-months of previous virologic suppression on a non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimen from two prospective cohorts in France and North America. We assessed the risk of virologic rebound, defined as HIV RNA of >400 copies/mL according to several MEMS adherence measurements. Seventy two subjects were studied, five of them experienced virologic rebound. Subjects with and without virologic rebound had similar baseline characteristics including treatment durations, regimen (efavirenz vs nevirapine), and dosing schedule. Each 10% increase in average adherence decreased the risk of virologic rebound (OR = 0.56; 95% confidence interval (CI) [0.37, 0.81], P<0.002). Each additional consecutive day off therapy for the longest treatment interruption (OR = 1.34; 95%CI [1.15, 1.68], P<0.0001) and each additional treatment interruption for more than 2 days (OR = 1.38; 95%CI [1.13, 1.77], P<0.002) increased the risk of virologic rebound. In those with low-to-moderate adherence (i.e. <80%), treatment interruption duration (16.2 days versus 6.1 days in the control group, P<0.02), but not average adherence (53.1% vs 55.9%, respectively, P = 0.65) was significantly associated with virologic rebound.
Conclusions: Sustained treatment interruption may pose a greater risk of virologic rebound on NNRTI therapy than the same number of interspersed missed doses at low-to-moderate adherence.
Conflict of interest statement
Figures

References
-
- Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133:21–30. - PubMed
-
- Parienti JJ, Massari V, Descamps D, Vabret A, Bouvet E, et al. Predictors of virologic failure and resistance in HIV-infected patients treated with nevirapine- or efavirenz-based antiretroviral therapy. Clin Infect Dis. 2004;38:1311–1316. - PubMed
-
- Bangsberg DR, Perry S, Charlebois ED, Clark RA, Roberston M, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. Aids. 2001;15:1181–1183. - PubMed
-
- Hogg RS, Heath K, Bangsberg D, Yip B, Press N, et al. Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. Aids. 2002;16:1051–1058. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
