

Quantitative evaluation of oxygenation in venous vessels using T2-Relaxation-Under-Spin-Tagging MRI
- PMID: 18666116
- PMCID: PMC2587050
- DOI: 10.1002/mrm.21627
Quantitative evaluation of oxygenation in venous vessels using T2-Relaxation-Under-Spin-Tagging MRI
Abstract
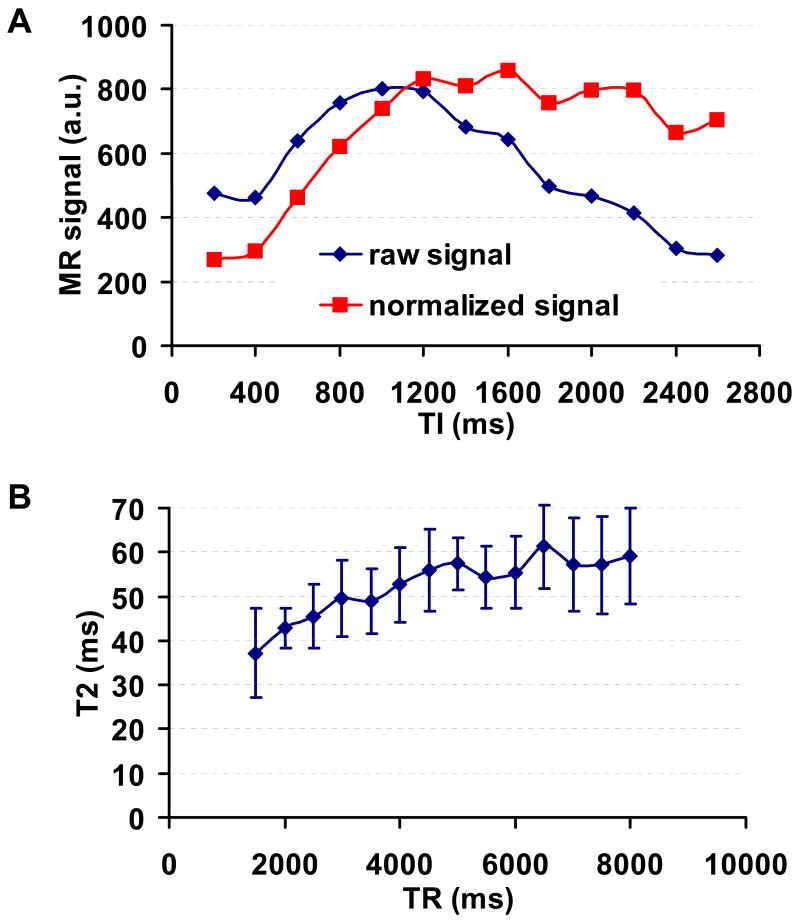
Noninvasive measurement of cerebral venous oxygenation can serve as a tool for better understanding fMRI signals and for clinical evaluation of brain oxygen homeostasis. In this study a novel technique, T2-Relaxation-Under-Spin-Tagging (TRUST) MRI, is developed to estimate oxygenation in venous vessels. This method uses the spin labeling principle to automatically isolate pure blood signals from which T2 relaxation times are determined using flow-insensitive T2-preparation pulses. The blood T2 is then converted to blood oxygenation using a calibration plot. In vivo experiments gave a baseline venous oxygenation of 64.8 +/- 6.3% in sagittal sinus in healthy volunteers (n = 24). Reproducibility studies demonstrated that the standard deviation across trials was 2.0 +/- 1.1%. The effects of repetition time and inversion time selections were investigated. The TRUST technique was further tested using various physiologic challenges. Hypercapnia induced an increase in venous oxygenation by 13.8 +/- 1.1%. On the other hand, caffeine ingestion resulted in a decrease in oxygenation by 7.0 +/- 1.8%. Contrast agent infusion (Gd-DTPA, 0.1 mmol/kg) reduced venous blood T2 by 11.2 ms. The results of this study show that TRUST MRI is a useful technique for quantitative assessment of blood oxygenation in the brain.
(c) 2008 Wiley-Liss, Inc.
Figures




References
-
- Nagdyman N, Fleck T, Schubert S, Ewert P, Peters B, Lange PE, Abdul-Khaliq H. Comparison between cerebral tissue oxygenation index measured by near-infrared spectroscopy and venous jugular bulb saturation in children. Intensive Care Med. 2005;31:846–850. - PubMed
-
- Coles JP, Minhas PS, Fryer TD, Smielewski P, Aigbirihio F, Donovan T, Downey SP, Williams G, Chatfield D, Matthews JC, Gupta AK, Carpenter TA, Clark JC, Pickard JD, Menon DK. Effect of hyperventilation on cerebral blood flow in traumatic head injury: clinical relevance and monitoring correlates. Crit Care Med. 2002;30:1950–1959. - PubMed
-
- Haacke EM, Lai S, Reichenbach JR, Kuppusamy K, Hoogenraad FG, Takeichi H, Lin W. In vivo measurement of blood oxygen saturation using magnetic resonance imaging: a direct validation of the blood oxygen level dependent concept in functional brain imaging. Human Brain Mapping. 1997;5:341–346. - PubMed
-
- Fox PT, Raichle ME, Mintun MA, Dence C. Nonoxidative glucose consumption during focal physiologic neural activity. Science. 1988;241:462–464. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
