

Resection and survival in glioblastoma multiforme: an RTOG recursive partitioning analysis of ALA study patients
- PMID: 18667747
- PMCID: PMC2719000
- DOI: 10.1215/15228517-2008-052
Resection and survival in glioblastoma multiforme: an RTOG recursive partitioning analysis of ALA study patients
Abstract
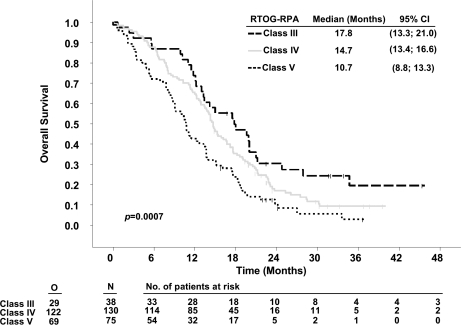
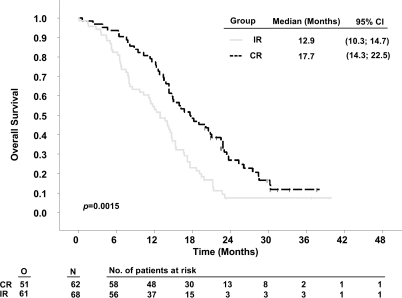
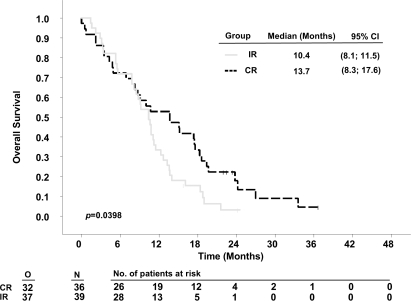
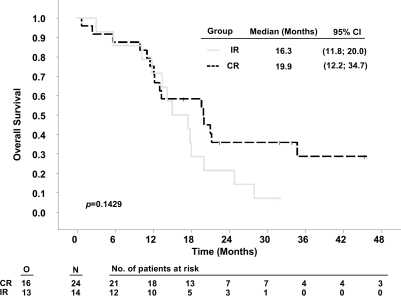
The benefit of cytoreductive surgery for glioblastoma multiforme (GBM) is unclear, and selection bias in past series has been observed. The 5-aminolevulinic acid (ALA) study investigated the influence of fluorescence-guided resections on outcome and generated an extensive database of GBM patients with optimized resections. We evaluated whether the Radiation Therapy Oncology Group recursive partitioning analysis (RTOG-RPA) would predict survival of these patients and whether there was any benefit from extensive resections depending on RPA class. A total of 243 per-protocol patients with newly diagnosed GBM were operated on with or without ALA and treated by radiotherapy. Postoperative MRI was obtained in all patients. Patients were allocated into RTOG-RPA classes III-V based on age, KPS, neurological condition, and mental status (as derived from the NIH Stroke Scale). Median overall survival among RPA classes III, IV, and V was 17.8, 14.7, and 10.7 months, respectively, with 2-year survival rates of 26%, 12%, and 7% (p = 0.0007). Stratified for degree of resection, survival of patients with complete resections was clearly longer in RPA classes IV and V (17.7 months vs. 12.9 months, p = 0.0015, and 13.7 months vs. 10.4 months, p = 0.0398; 2-year rates: 21.0% vs. 4.4% and 11.1% vs. 2.6%, respectively), but was not in the small subgroup of RPA class III patients (19.3 vs. 16.3 months, p = 0.14). Survival of patients from the ALA study is correctly predicted by the RTOG-RPA classes. Differences in survival depending on resection status, especially in RPA classes IV and V, support a causal influence of resection on survival.
Figures
References
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ, ALA Glioma Study Group Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol. 2006;7:392–401. - PubMed
-
- Albert FK, Forsting M, Sartor K, Adams HP, Kunze S. Early postoperative magnetic resonance imaging after resection of malignant glioma: objective evaluation of residual tumor and its influence on regrowth and prognosis. Neurosurgery. 1994;34:45–60. - PubMed
-
- Barker FG, II, Prados MD, Chang SM, et al. Radiation response and survival time in patients with glioblastoma multiforme. J Neurosurg. 1996;84:442–448. - PubMed
-
- Kowalczuk A, Macdonald RL, Amidei C, et al. Quantitative imaging study of extent of surgical resection and prognosis of malignant astrocytomas. Neurosurgery. 1997;41:1028–1036. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
