

Review
doi: 10.1002/ana.21430.
Rapidly progressive dementia
Affiliations
- PMID: 18668637
- PMCID: PMC2647859
- DOI: 10.1002/ana.21430
Item in Clipboard
Review
Rapidly progressive dementia
Ann Neurol.
2008 Jul.
Abstract
In contrast with more common dementing conditions that typically develop over years, rapidly progressive dementias can develop subacutely over months, weeks, or even days and be quickly fatal. Because many rapidly progressive dementias are treatable, it is paramount to evaluate and diagnose these patients quickly. This review summarizes recent advances in the understanding of the major categories of RPD and outlines efficient approaches to the diagnosis of the various neurodegenerative, toxic-metabolic, infectious, autoimmune, neoplastic, and other conditions that may progress rapidly.
Figures
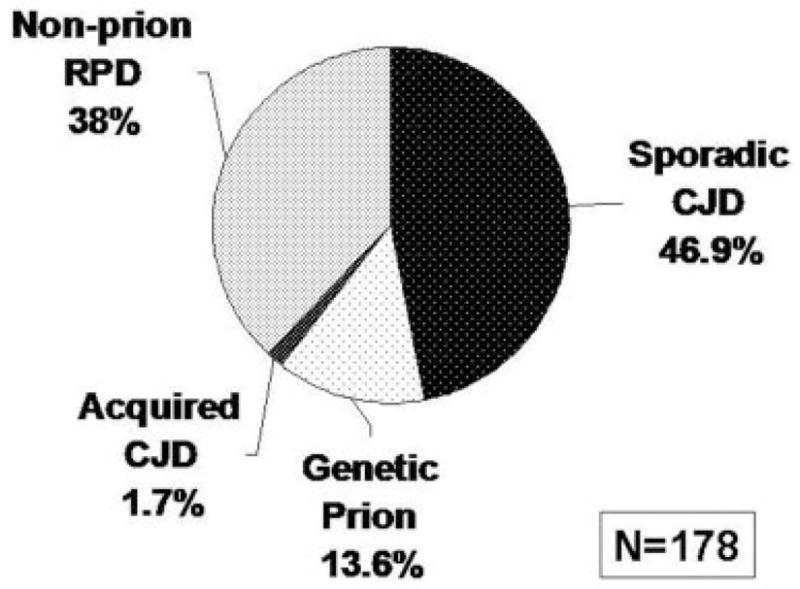
Diagnosis of University of California, San Francisco (UCSF)–evaluated rapidly progressive dementia (RPD) referrals (N =178) from August 2001 to September 2007. Pie chart showing the percentile of broad categories for final diagnoses of patients with suspected Creutzfeldt–Jakob disease (CJD) or other RPDs. Note that in many cases referred with suspected prion disease, a nonprion diagnosis was made.
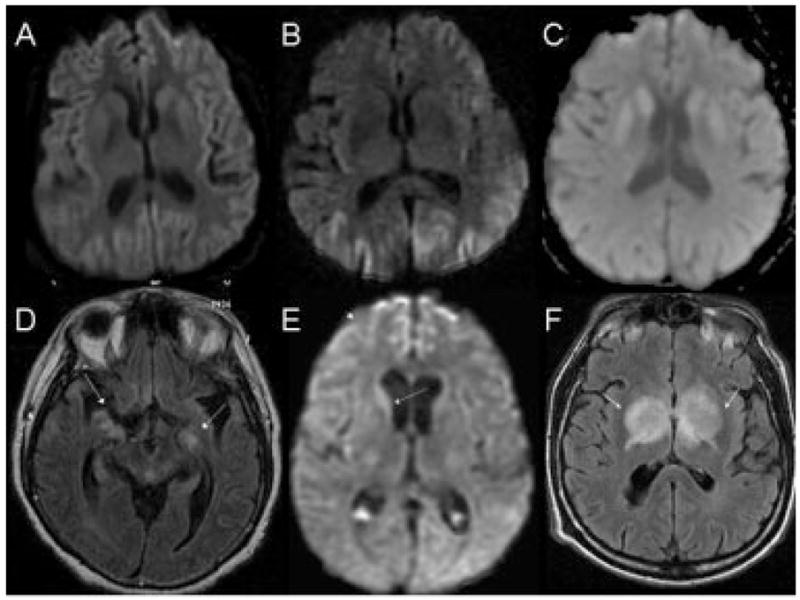
Brain magnetic resonance images (MRIs) in sporadic Creutzfeldt–Jakob disease (CJD) (A–C) and nonprion rapidly progressive dementias (RPDs) (D–F). Sporadic CJD axial diffusion-weighted imaging (DWI) with both cortical and striatal hyperintensity (A), only cortical (cortical ribboning) hyperintensity (B), and only striatal hyperintensity (C). Fluid-attenuated inversion recovery (FLAIR) MRIs (not shown) showed less hyperintensity than DWI sporadic CJD. Axial FLAIR MRI of patient with pathology-proved meningoencephalitis (D) showing extensive, patchy, T2-weighted white matter hyperintensity (arrows) that was variably contrast enhancing (not shown). Enterovirus was identified through the California Encephalitis Project by reverse transcription-polymerase chain reaction of brain biopsy tissue. DWI axial MRI of a patient with systemic sarcoid (E). Initial diagnosis suggested CJD because of caudate hyperintensity (arrow) and right frontal cortical ribboning (arrowhead). The apparent diffusion coefficient map (not shown), however, did not suggest restricted diffusion, and a lung node biopsy showed sarcoid. Axial FLAIR MRI of an RPD patient with parkinsonism (F). Arrows point to the masses in the bilateral deep nuclei. Note the mass effect with edema (arrows). The lesions were hypodense on T1 and showed some gadolinium enhancement (not shown). Brain biopsy showed a B-cell primary central nervous system lymphoma.
References
-
- Roberson ED, Hesse JH, Rose KD, et al. Frontotemporal dementia progresses to death faster than Alzheimer disease. Neurology. 2005;65:719–725. - PubMed
-
- Rascovsky K, Salmon DP, Lipton AM, et al. Rate of progression differs in frontotemporal dementia and Alzheimer disease. Neurology. 2005;65:397–403. - PubMed
-
- Cercy SP, Bylsma FW. Lewy bodies and progressive dementia: a critical review and metaanalysis. J Int Neuropsychol Soc. 1997;3:179–194. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
