

Airway bypass improves the mechanical properties of explanted emphysematous lungs
- PMID: 18669815
- PMCID: PMC2577725
- DOI: 10.1164/rccm.200712-1832OC
Airway bypass improves the mechanical properties of explanted emphysematous lungs
Abstract
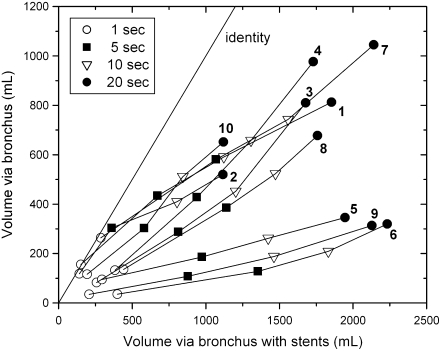
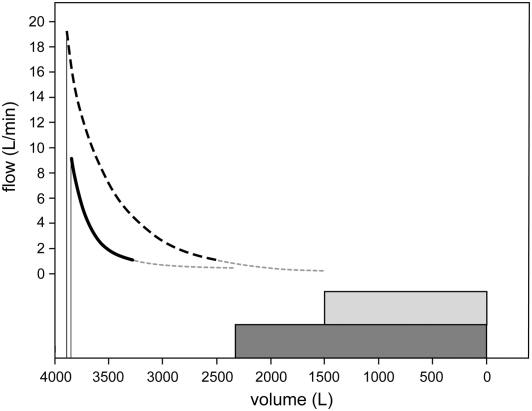
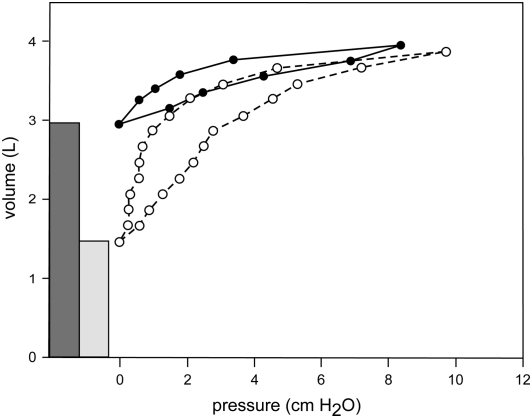
Rationale: By creating artificial communications through bronchial walls into the parenchyma of explanted lungs (airway bypass), we expect to decrease the amount of gas trapped and to increase the rate and volume of air expelled during forced expirations.
Objectives: To describe the mechanism by which airway bypass improves the mechanical properties of the emphysematous lung.
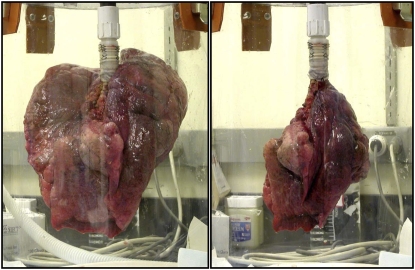
Methods: Lung compartments and mechanics were measured before and after airway bypass, which was created by placement of three or four stent-supported fenestrations in 10 emphysematous lungs removed at transplantation surgery.
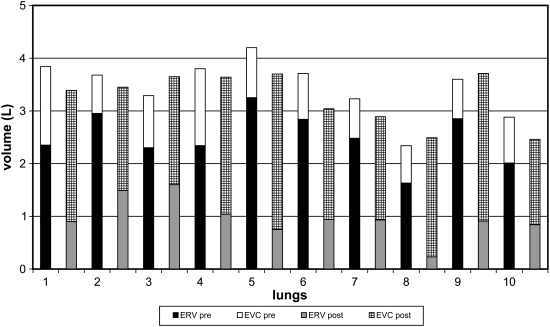
Measurements and main results: Minimal volume after passive deflation decreased by a mean of 1.54 L (range, 0.7-2.5 L) or 60% (range, 37-86%). Explanted VC increased by 1.30 L or 132% (range, 78-318%). Maximal expiratory flows and volumes increased. Flow resistance decreased.
Conclusions: Because these data show that airway bypass improves the mechanics of breathing in severely emphysematous lungs in vitro, there is now strong empirical support that this procedure can improve ventilatory function in patients by reducing gas trapping and flow resistance.
Figures
References
-
- Lausberg HF, Chino K, Patterson GA, Meyers BF, Toeniskoetter PD, Cooper JD. Bronchial fenestration improves expiratory flow in emphysematous human lungs. Ann Thorac Surg 2003;75:393–397. - PubMed
-
- Rendina EA, De Giacomo T, Venuta F, Coloni GF, Meyers BF, Patterson GA, Cooper JD. Feasibility and safety of the airway bypass procedure for patients with emphysema. J Thorac Cardiovasc Surg 2003;125:1294–1299. - PubMed
-
- Choong CK, Haddad FJ, Gee EY, Cooper JD. Feasibility and safety of airway bypass stent placement and influence of topical mitomycin C on stent patency. J Thorac Cardiovasc Surg 2005;129:632–638. - PubMed
-
- Choong CK, Phan L, Massetti P, Haddad FJ, Martinez C, Roschak E, Cooper JD. Prolongation of patency of airway bypass stents with use of drug-eluting stents. J Thorac Cardiovasc Surg 2006;131:60–64. - PubMed
-
- Macklem PT, Cardoso P, Snell G, Hopkins P, Sybrecht GW, Pierce J, Cooper J. Airway bypass: a new treatment for emphysema. Proc Am Thorac Soc 2006;3:A726.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
