

Atrial-selective sodium channel blockers: do they exist?
- PMID: 18670368
- PMCID: PMC2574832
- DOI: 10.1097/FJC.0b013e31817618eb
Atrial-selective sodium channel blockers: do they exist?
Abstract
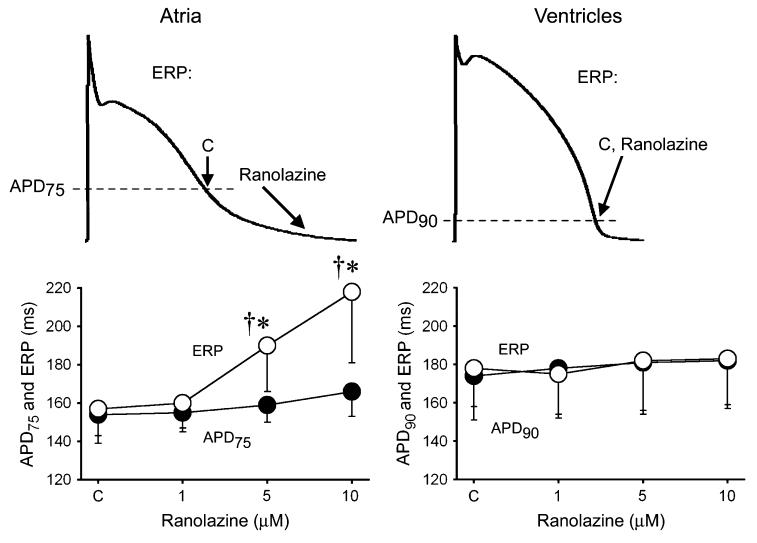
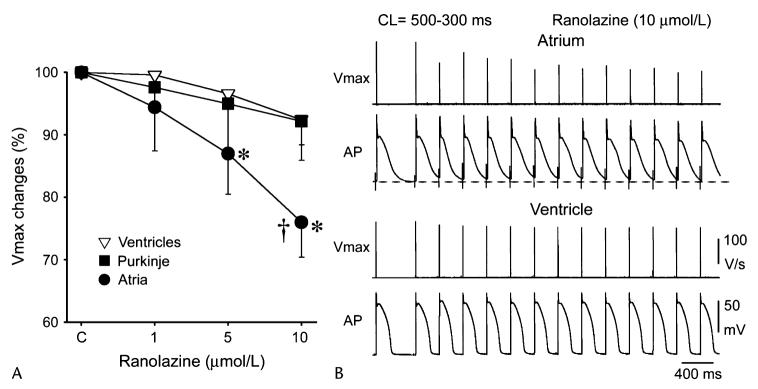
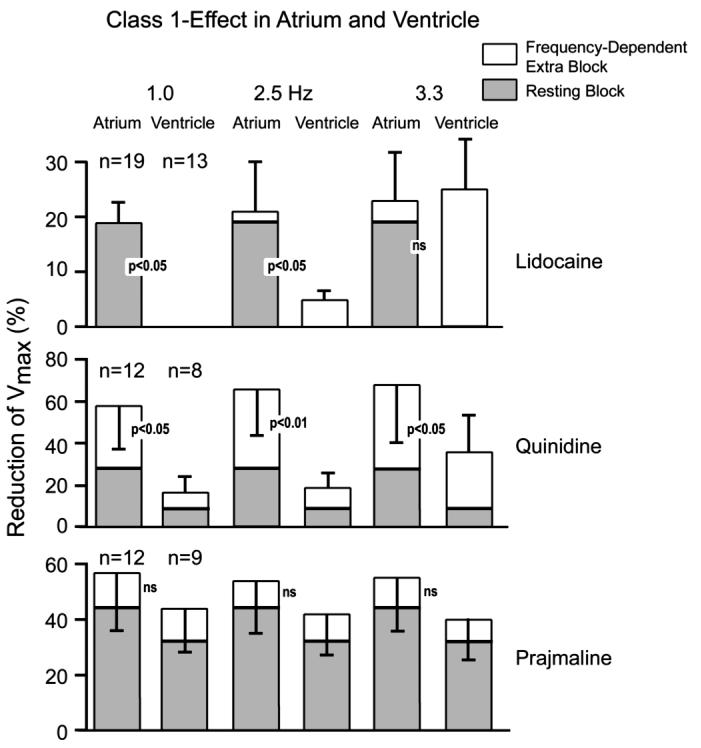
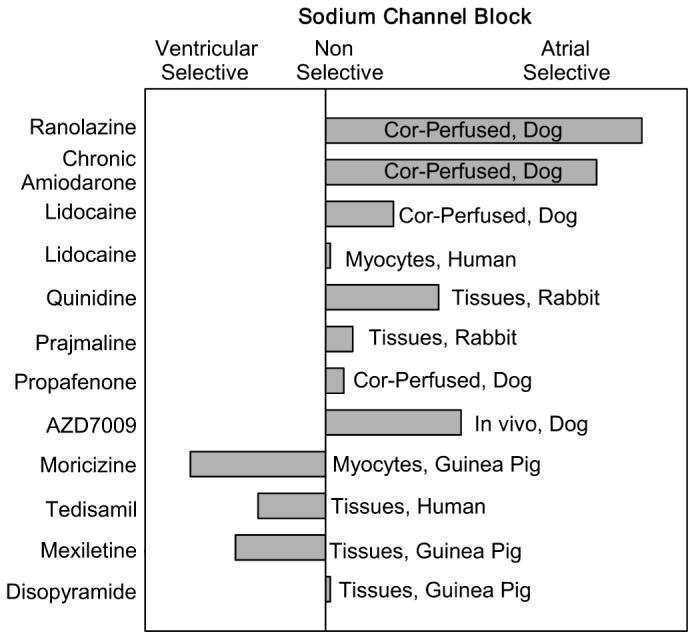
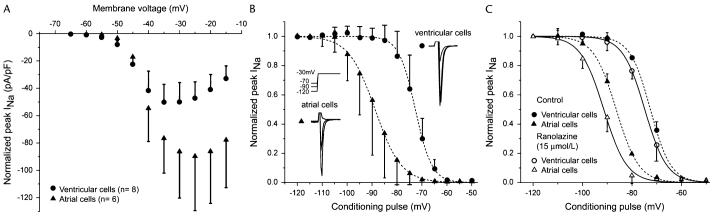
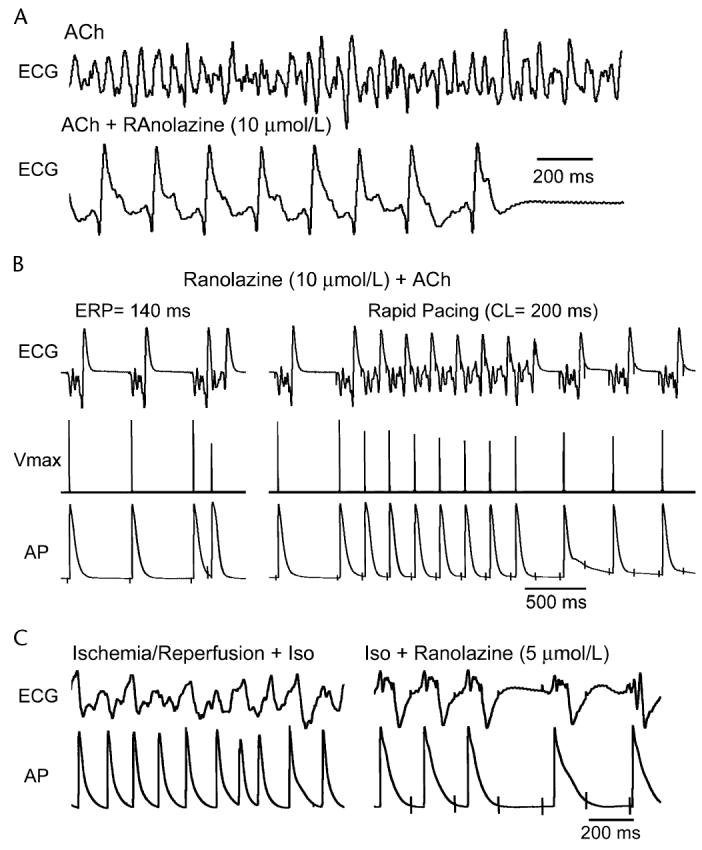
The risk of developing severe ventricular arrhythmias and/or organ toxicity by currently available drugs used to treat atrial fibrillation (AF) has prompted the development of atrial-selective antiarrhythmic agents. Until recently the principal focus has been on development of agents that selectively inhibit the ultra-rapid delayed rectifier outward potassium channels (I Kur), taking advantage of the presence of these channels in atria but not ventricles. Recent experimental studies have demonstrated important atrioventricular differences in biophysical properties of the sodium channel and have identified sodium channel blockers such as ranolazine and chronic amiodarone that appear to take advantage of these electrophysiologic distinctions and act to specifically or predominantly depress sodium channel-mediated parameters in "healthy" canine atria versus ventricles. Atrial-selective/predominant sodium channel blockers such as ranolazine effectively suppress AF in experimental models of AF involving canine isolated right atrial preparations at concentrations that produce little to no effect on ventricular electrophysiologic parameters. These findings point to atrial-selective sodium channel block as a new strategy for the management of AF. The present review examines our current understanding of atrioventricular distinctions between atrial and ventricular sodium channels and our understanding of the basis for atrial selectively of the sodium channel blockers. A major focus will be on the ability of the atrial-selective sodium channel blocking properties of these agents, possibly in conjunction with I Kur and/or I Kr blocking properties, to suppress and prevent the reinduction of AF.
Figures
References
-
- Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation—Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation) J Am Coll Cardiol. 2006;48:854–906. - PubMed
-
- Nattel S, Carlsson L. Innovative approaches to anti-arrhythmic drug therapy. Nat Rev Drug Discov. 2006;5:1034–1049. - PubMed
-
- Blaauw Y, Gogelein H, Tieleman RG, et al. “Early” class III drugs for the treatment of atrial fibrillation: Efficacy and atrial selectivity of AVE0118 in remodeled atria of the goat. Circulation. 2004;110:1717–1724. - PubMed
-
- Goldstein RN, Khrestian C, Carlsson L, et al. Azd7009: A new anti-arrhythmic drug with predominant effects on the atria effectively terminates and prevents reinduction of atrial fibrillation and flutter in the sterile pericarditis model. J Cardiovasc Electrophysiol. 2004;15:1444–1450. - PubMed
-
- Fedida D, Orth PM, Chen JY, et al. The mechanism of atrial antiarrhythmic action of RSD1235. J Cardiovasc Electrophysiol. 2005;16:1227–1238. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
