

Pulmonary hypertension associated with lung transplantation obliterative bronchiolitis and vascular remodeling of the allograft
- PMID: 18671677
- PMCID: PMC4207285
- DOI: 10.1111/j.1600-6143.2008.02338.x
Pulmonary hypertension associated with lung transplantation obliterative bronchiolitis and vascular remodeling of the allograft
Abstract
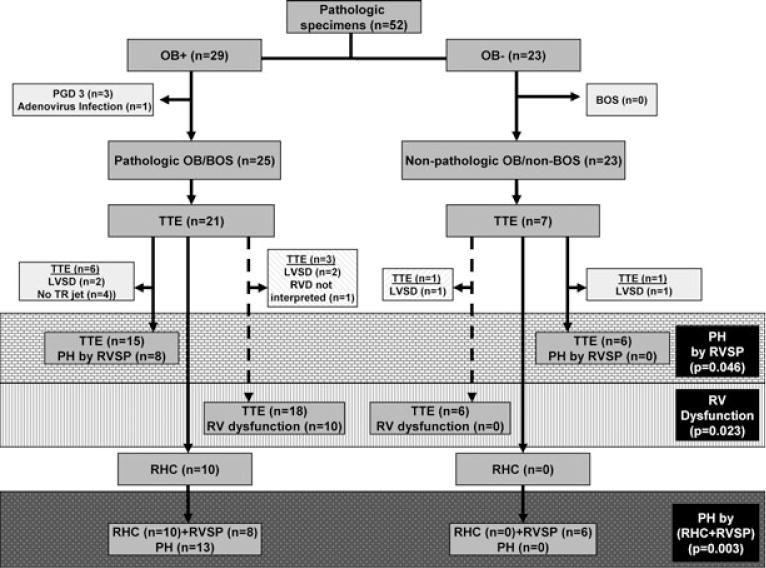
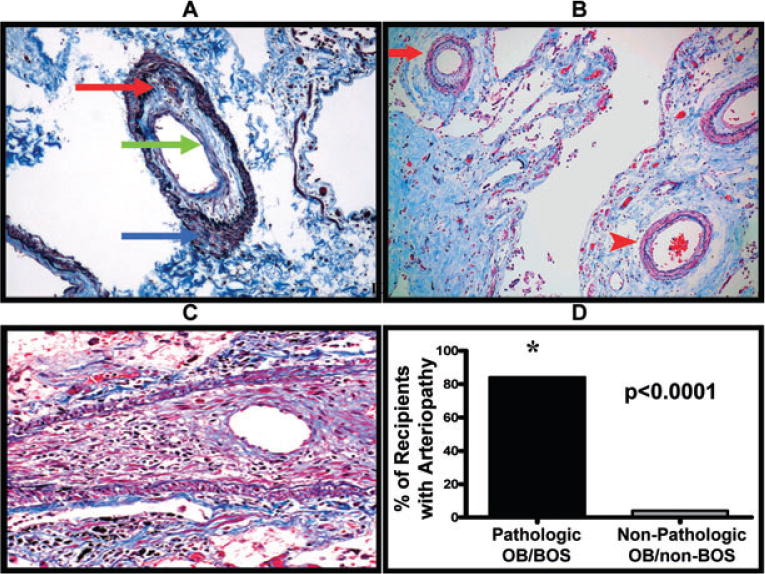
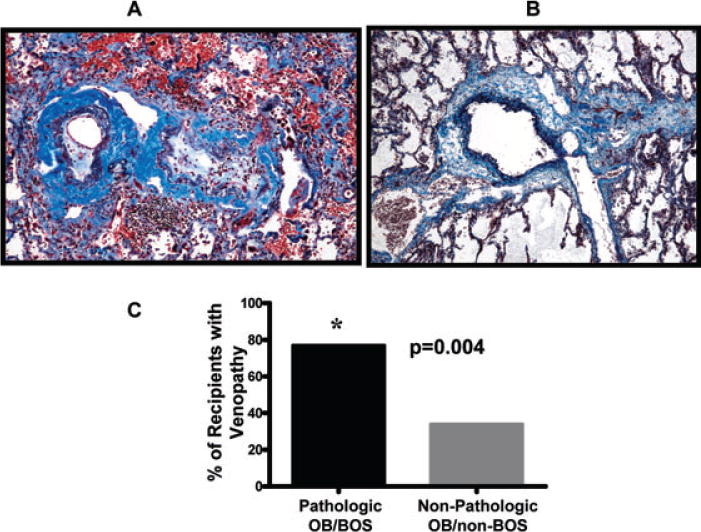
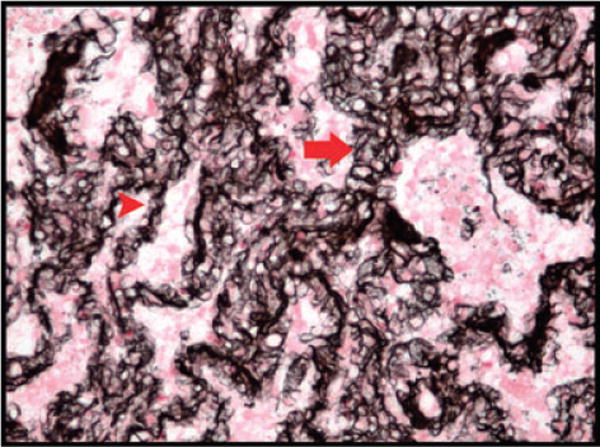
Pathologic obliterative bronchiolitis (OB)/Bronchiolitis obliterans syndrome (pathologic OB/BOS) is the major obstacle to long-term survival post-lung transplantation (LT). Our group has demonstrated that pulmonary hypertension (PH) complicates the course of chronic inflammatory lung diseases that have similarities to pathologic OB/BOS and that vascular remodeling of the bronchial circulation occurs during BOS. Consequently, we hypothesized that PH is associated with pathologic OB/BOS and may result from a vasculopathy of the allograft pulmonary circulation. We conducted a single-center, retrospective study and examined the presence of PH and vasculopathy in patients with pathologic OB/BOS. Fifty-two pathologic specimens post-LT were recovered from January 10, 1997 to January 5, 2007 and divided into two groups, those with and without pathologic OB/BOS.PH was defined as a mean pulmonary artery pressure (mPAP) > 25 mmHg by right heart catheterization (RHC) or right ventricular systolic pressure (RVSP) > or = 45 mmHg by transthoracic echocardiogram (TTE). PH was more prevalent in those LT recipients with pathologic OB/BOS (72% vs. 0%, p = 0.003). Furthermore, pulmonary arteriopathy and venopathy were more prevalent in patients with pathologic OB/BOS (84% vs. 4%, p < 0.0001, and 77% vs. 35%, p = 0.004, respectively). PH is common in LT recipients with pathologic OB/BOS and is associated with a vasculopathy of the allograft pulmonary circulation.
Figures
References
-
- Nadrous HF, Pellikka PA, Krowka MJ, et al. The impact of pulmonary hypertension on survival in patients with idiopathic pulmonary fibrosis. Chest. 2005;128(6 Suppl):616S–617S. - PubMed
-
- Shorr AF, Davies DB, Nathan SD. Outcomes for patients with sarcoidosis awaiting lung transplantation. Chest. 2002;122:233–238. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
