

Family physician and endocrinologist coordination as the basis for diabetes care in clinical practice
- PMID: 18671870
- PMCID: PMC2518542
- DOI: 10.1186/1472-6823-8-9
Family physician and endocrinologist coordination as the basis for diabetes care in clinical practice
Abstract
Background: To estimate the proportion of diabetic patients (DPts) with peripheral vascular disease treated at a primary health care site after an endocrinologist-based intervention, who meet ATP III and Steno targets of metabolic control, as well as to compare the outcome with the results of the patients treated by endocrinologists.
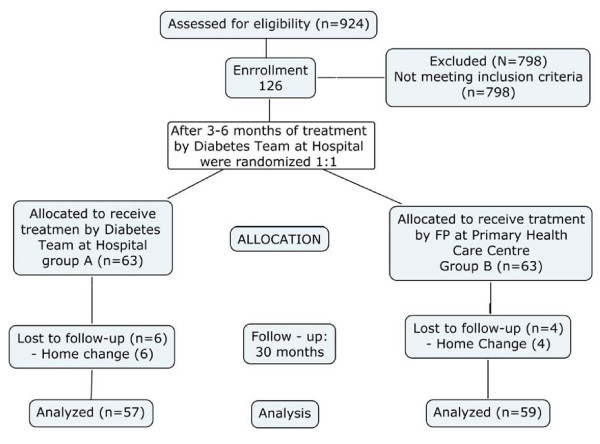
Methods: A controlled, prospective over 30-months period study was conducted in area 7 of Madrid. One hundred twenty six eligible diabetic patients diagnosed as having peripheral vascular disease between January 2003 and June 2004 were included in the study. After a treatment period of three months by the Diabetes team at St Carlos Hospital, 63 patients were randomly assigned to continue their follow up by diabetes team (Group A) and other 63 to be treated by the family physicians (FP) at primary care level with continuous diabetes team coordination (Group B). 57 DPts from Group A and 59 from Group B, completed the 30 months follow-up period. At baseline both groups were similar in age, weight, time from diagnosis and metabolic control. The main outcomes of this study were the proportion of patients meeting ATP III and Steno goals for HbA1c (%), Cholesterol, HDL cholesterol, LDL cholesterol, triglycerides, blood pressure, albumine-to-creatinine excretion ratio (ACR), body mass index (BMI), waist circumference (WC), anti-aggregation treatment and smoking status.
Results: At the end of the follow up, no differences were found between the groups. More than 37% of diabetic patients assigned to be treated by FP achieved a HbA1c < 6.5%, more than 50% a ACR < 30 mg/g, and more than 80% reached low risk values for cholesterol, LDL cholesterol, triglycerides, diastolic blood pressure and were anti-aggregated, and 12% remained smokers. In contrast, less than 45% achieved a systolic blood pressure < 130 mm Hg, less than 12% had a BMI < 25 Kg.m-2 (versus 23% in group A; p < 0.05) and 49%/30% (men/women) had a waist circumference of low risk.
Conclusion: Improvements in metabolic control among diabetic patients with peripheral vascular disease treated at a primary health care setting is possible, reaching similar results to the patients treated at a specialized level. Despite such an improvement, body weight control remains more than poor in both levels, mainly at primary care level. General practitioner and endocrinologist coordination care may be important to enhance diabetes management in primary care settings.
Trial registration: Clinical Trial number ISRCTN75037597.
References
-
- Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, Kojima Y, Furoyoshi N, Shichiri M. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28:103–117. doi: 10.1016/0168-8227(95)01064-K. - DOI - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;353:837–853. - PubMed
LinkOut - more resources
Full Text Sources
