

Diabetic neuropathy in older adults
- PMID: 18672180
- PMCID: PMC2706706
- DOI: 10.1016/j.cger.2008.03.011
Diabetic neuropathy in older adults
Abstract
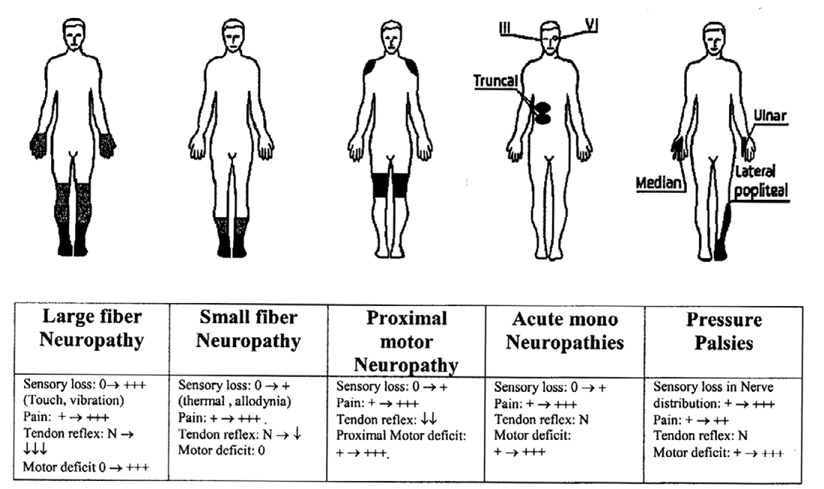
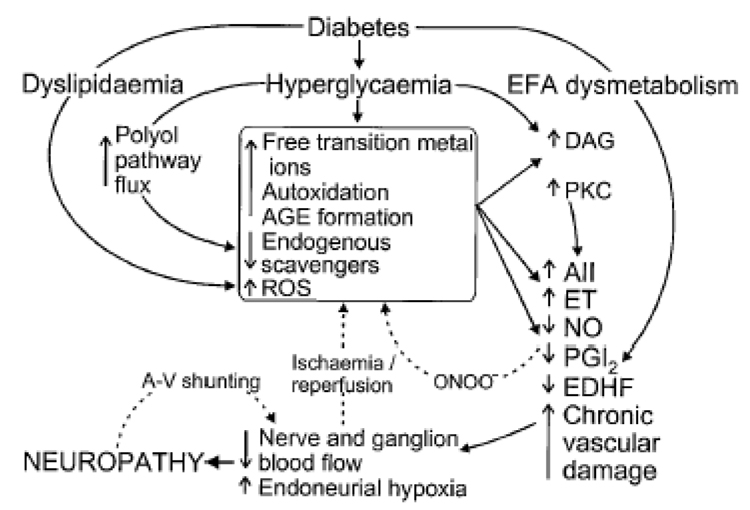
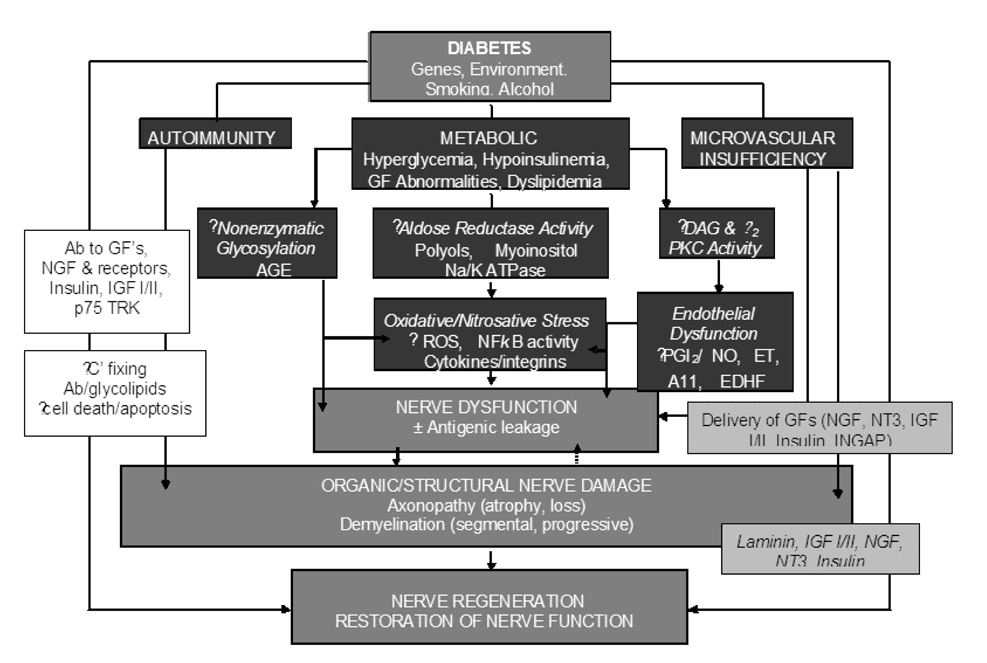
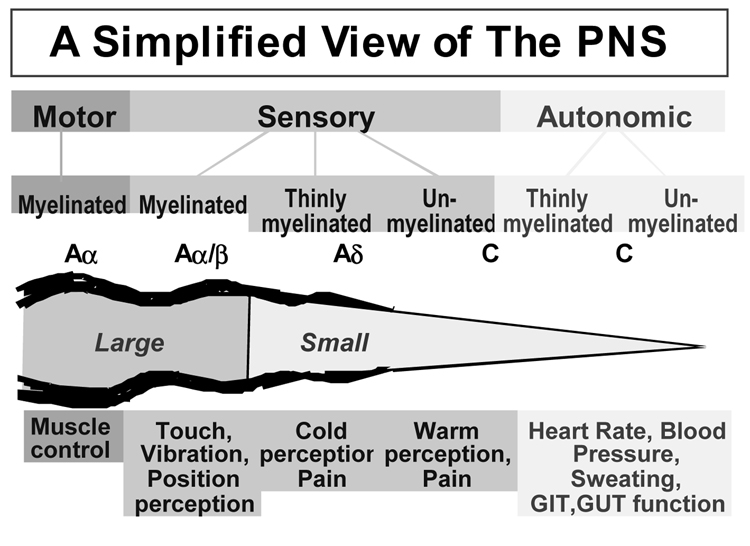
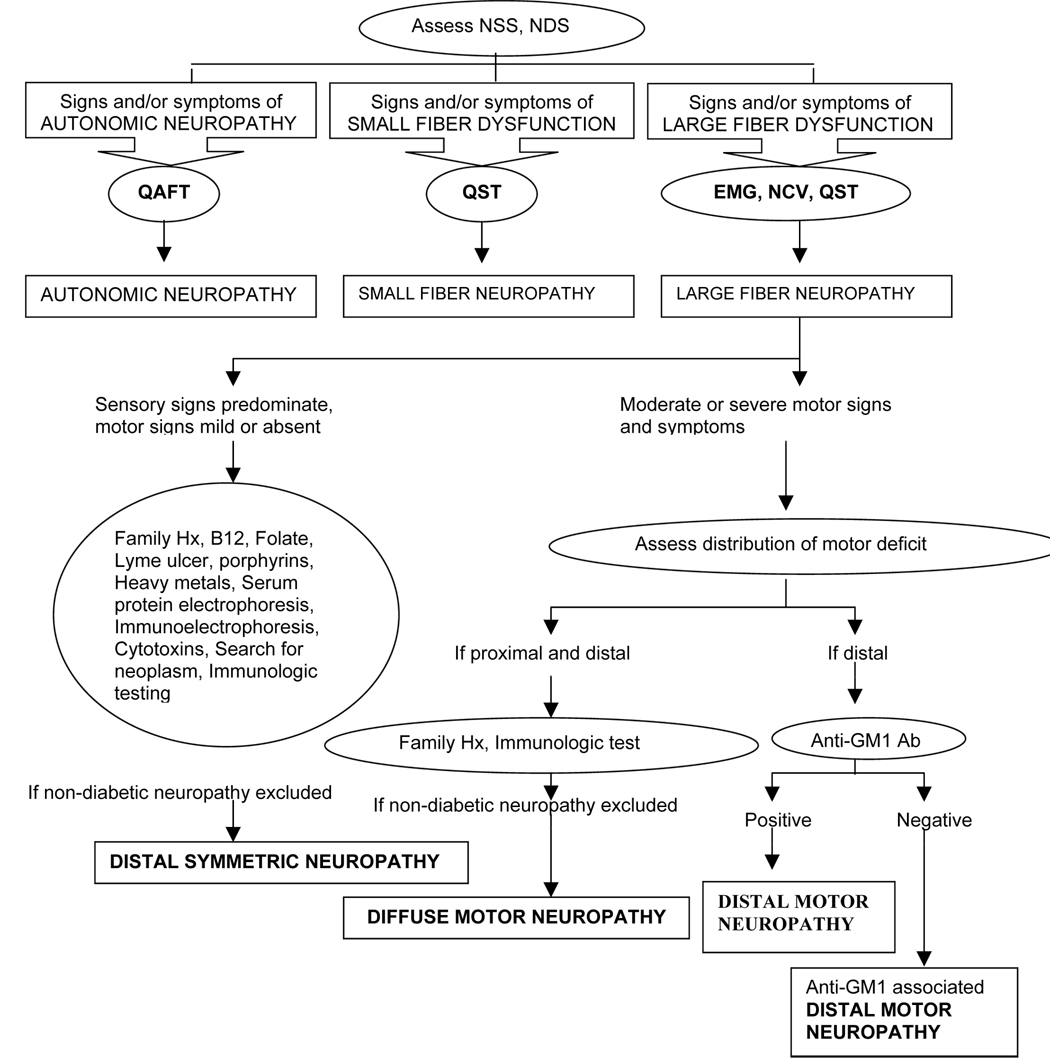
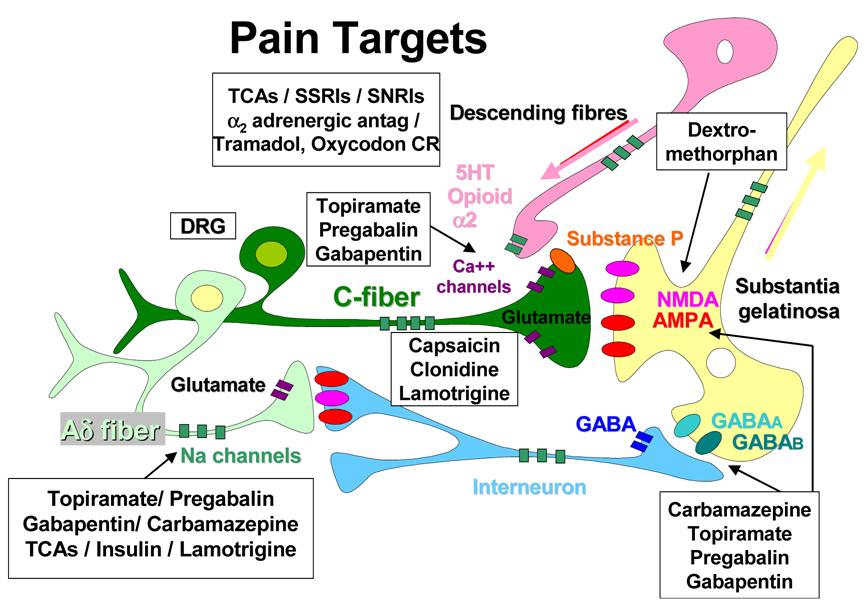
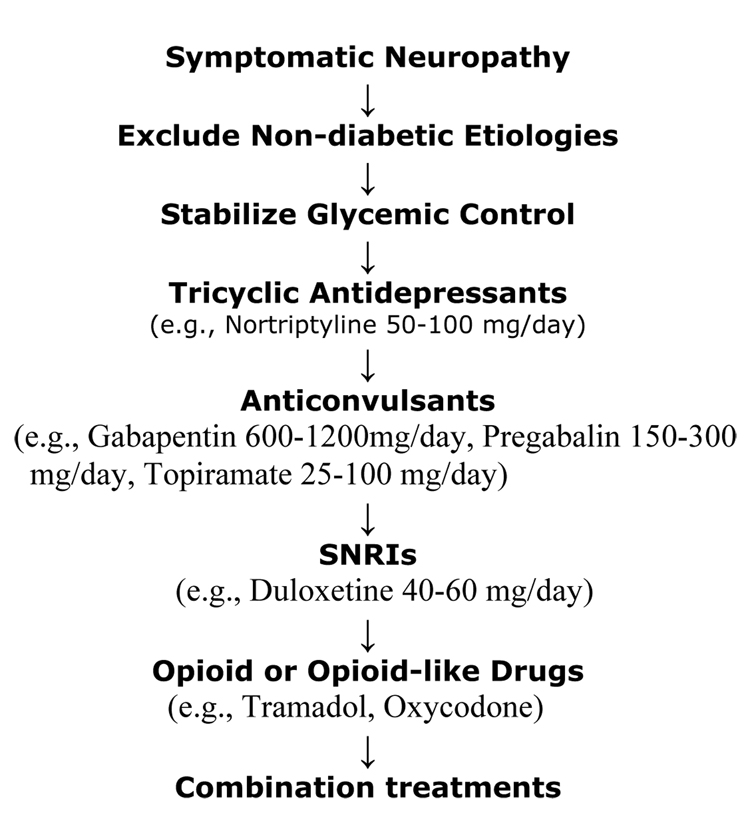
Diabetic neuropathy is a heterogeneous disease with diverse pathology. Recognition of the clinical homolog of these pathologic processes is necessary in achieving appropriate intervention. Treatment should be individualized so the particular manifestation and underlying pathogenesis of each patient's clinical presentation are considered. In older adults, special care should be taken to manage pain while optimizing daily function and mobility, with the fewest adverse medication side effects. Older adults are at great risk for falling and fractures because of instability and weakness, and require strength exercises and coordination training. Ultimately agents that address large fiber dysfunction will be essential to reduce the gross impairment of quality of life and activities of daily living that neuropathy visits older people who have diabetes.
Figures
References
-
- Vinik AI, Mitchell BD, Leichter SB, Wagner AL, O'Brian JT, Georges LP. Epidemiology of the Complications of Diabetes. In: Leslie RDG, Robbins DC, editors. Diabetes: Clinical Science in Practice. Cambridge, United Kingdom: Cambridge University Press; 1995. pp. 221–287.
-
- Knuiman M, Welborn T, McCann V, Stanton K, Constable I. Prevalence of diabetic complications in relation to risk factors. Diabetes. 1986;35:1332–1339. - PubMed
-
- Young MJ, Boulton AJM, MacLeod AF, Williams DRR, Sonksen PH. A multicenter study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia. 1993;36:1–5. - PubMed
-
- Holzer SE, Camerota A, Martens L, Cuerdon T, Crystal P, Zagari M. Costs and duration of care for lower extremity ulcers in patients with diabetes. Clin Ther. 1998;20:169–181. - PubMed
-
- Caputo GM, Cavanagh PR, Ulbrecht JS, Gibbons GW, Karchmer AW. Assessment and management of foot disease in patients with diabetes. N Engl J Med. 1994;331:854–860. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
