

Night vision symptoms and progression of age-related macular degeneration in the Complications of Age-related Macular Degeneration Prevention Trial
- PMID: 18672295
- PMCID: PMC2600589
- DOI: 10.1016/j.ophtha.2008.05.023
Night vision symptoms and progression of age-related macular degeneration in the Complications of Age-related Macular Degeneration Prevention Trial
Abstract
Objective: To describe baseline night vision symptoms and their association with >/=3-lines loss in visual acuity (VA), choroidal neovascularization (CNV), and geographic atrophy (GA).
Design: Cohort study within a multicenter randomized clinical trial.
Participants: A total of 1052 participants with >/=10 large (>125 mu) drusen and VA >/=20/40 in each eye.
Methods: At baseline, participants self-administered a 10-item Night Vision Questionnaire (NVQ-10). VA testing was performed at baseline, 6 months, and annually. One eye of each participant was randomly assigned to laser treatment, and the contralateral eye was assigned to observation. During follow-up, trained readers identified CNV on the basis of fluorescein angiograms and end point GA, defined as >1 disc area of new GA, based on color photographs. Evaluation was performed by repeated-measures logistic regression for NVQ-10 score as a risk factor for >/=3-lines loss in VA and by survival analysis for CNV and GA, with and without adjustment for participant and ocular characteristics. Evaluations were based on observed eyes and treated eyes, considered separately and combined.
Main outcome measures: A >/=3-lines loss in VA, development of CNV and end point GA.
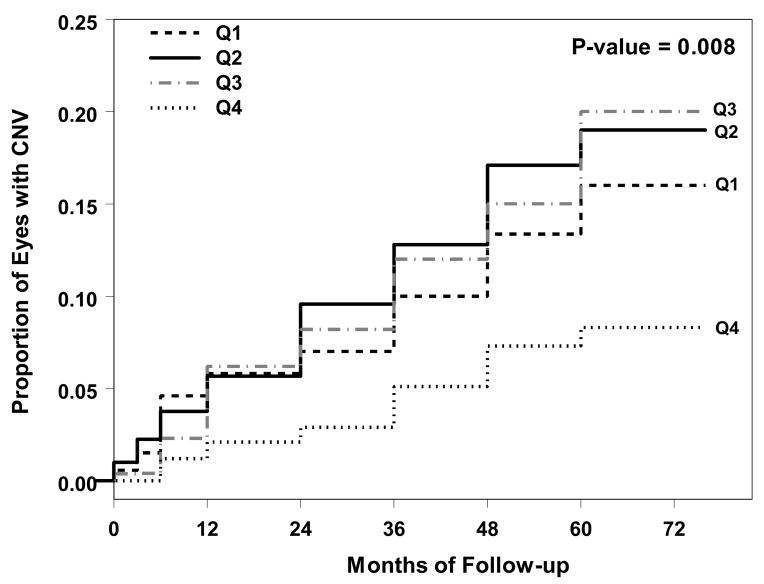
Results: At baseline, NVQ-10 scores ranged from 3 to 100 with a mean of 70 (100 corresponds to no night vision symptoms). Compared with participants with the best night vision (fourth quartile of scores), participants with the worst night vision (first quartile of scores) were at increased risk of >/=3-lines loss in VA in both observed and treated eyes; odds ratios (95% confidence interval) were 2.85 (1.85-4.39) and 2.00 (1.27-3.14), respectively. The relative risk for the first quartile versus the fourth quartile for development of GA was 4.18 (1.80-9.68) in observed eyes and 2.59 (1.13-5.95) in treated eyes. The relative risk for CNV incidence was 1.99 (1.12-3.54) in observed eyes and 1.33 (0.81-2.19) in treated eyes. These relationships were maintained after adjustment for baseline participant and ocular characteristics.
Conclusions: Participants who perceived the most problems in their night vision at baseline had an increased risk of >/=3-lines loss in VA, CNV, and GA. These associations are independent of established risk factors.
Figures



References
-
- Klein R, Peto T, Bird A, Vannewkirk MR. The epidemiology of age-related macular degeneration. Am J Ophthalmol. 2004;137:486–95. - PubMed
-
- Mohand-Said S, Hicks D, Leveillard T, et al. Rod-cone interactions: developmental and clinical significance. Prog Retin Eye Res. 2001;20:451–67. - PubMed
-
- Kosnik W, Winslow L, Kline D, et al. Visual changes in daily life throughout adulthood. J Gerontol. 1988;43:P63–70. - PubMed
-
- Kuyk T, Elliott JL. Visual factors and mobility in persons with age-related macular degeneration. J Rehabil Res Dev. 1999;36:303–12. - PubMed
-
- Mangione CM, Gutierrez PR, Lowe G, et al. Influence of age-related maculopathy on visual functioning and health-related quality of life. Am J Ophthalmol. 1999;128:45–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
