

The management of inflammation in periodontal disease
- PMID: 18673016
- PMCID: PMC2563957
- DOI: 10.1902/jop.2008.080173
The management of inflammation in periodontal disease
Abstract
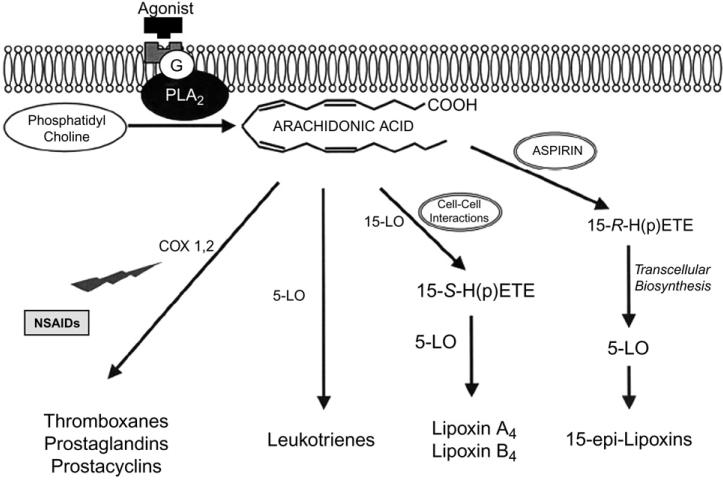
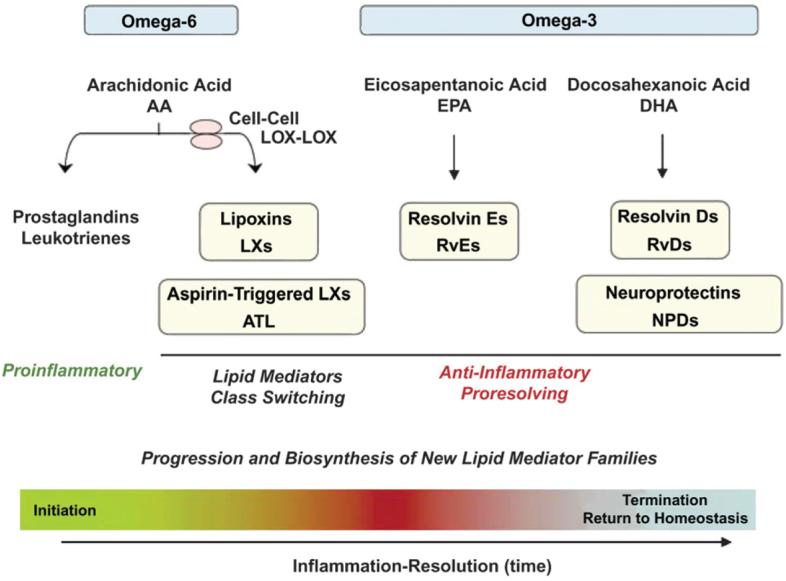
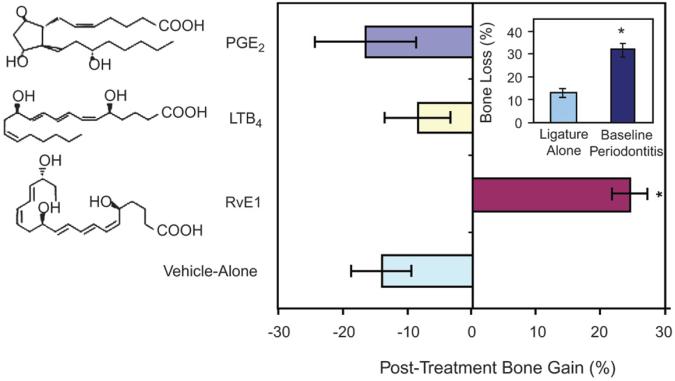
It has become clear in recent years that periodontitis is an inflammatory disease initiated by oral microbial biofilm. This distinction implies that it is the host response to the biofilm that destroys the periodontium in the pathogenesis of the disease. As our understanding of pathways of inflammation has matured, a better understanding of the molecular basis of resolution of inflammation has emerged. Resolution of inflammation is an active, agonist-mediated, well-orchestrated return of tissue homeostasis. There is an important distinction between anti-inflammation and resolution; anti-inflammation is pharmacologic intervention in inflammatory pathways, whereas resolution is biologic pathways restoring homeostasis. A growing body of research suggests that chronic inflammatory periodontal disease involves a failure of resolution pathways to restore homeostasis. This article reviews the resolution of inflammation in the context of periodontal disease and the potential for the modification of resolution pathways for the prevention and treatment of periodontal diseases. Proof-of-concept studies in the 1980s demonstrated that pharmacologic anti-inflammation prevented and slowed the progression of periodontal diseases in animals and man. However, the side-effect profile of such therapies precluded the use of non-steroidal anti-inflammatory drugs or other enzyme inhibitors or receptor antagonists in periodontal therapy. The isolation and characterization of resolving agonist molecules has opened a new area of research using endogenous lipid mediators of resolution as potential therapeutic agents for the management of inflammatory periodontitis. Work in animal models of periodontitis has revealed the potential of this therapeutic approach for its prevention and treatment and forced the reconsideration of our understanding of the pathogenesis of human periodontal diseases.
Figures
References
-
- Van Dyke TE, Serhan CN. Resolution of inflammation: A new paradigm for the pathogenesis of periodontal diseases. J Dent Res. 2003;82:82–90. - PubMed
-
- Van Dyke TE. Control of inflammation and periodontitis. Periodontol 2000. 2007;45:158–166. - PubMed
-
- Serhan CN. Novel omega–3-derived local mediators in anti-inflammation and resolution. Pharmacol Ther. 2005;105:7–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
