

Challenges in the prenatal and post-natal diagnosis of mediastinal cystic hygroma: a case report
- PMID: 18673546
- PMCID: PMC2518156
- DOI: 10.1186/1752-1947-2-256
Challenges in the prenatal and post-natal diagnosis of mediastinal cystic hygroma: a case report
Abstract
Introduction: Cystic hygroma is a benign congenital neoplasm that mostly presents as a soft-tissue mass in the posterior triangle of the neck. Pure mediastinal lesions are uncommon; the vast majority are asymptomatic and are an incidental finding in adulthood. The diagnosis is often made intra- or postoperatively. Prenatal identification is exceptional and post-natal diagnosis also proves challenging.
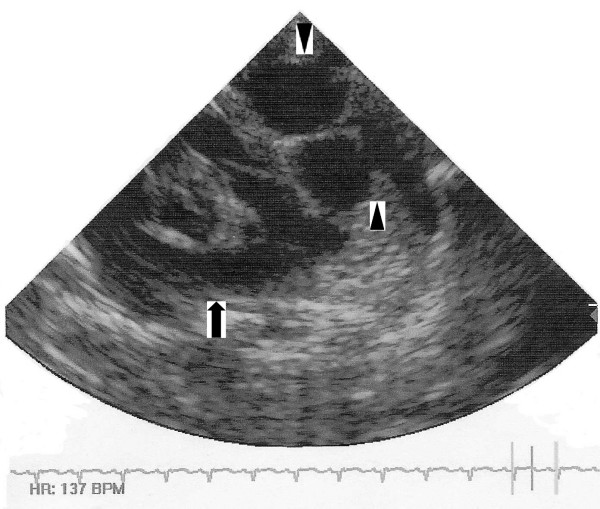
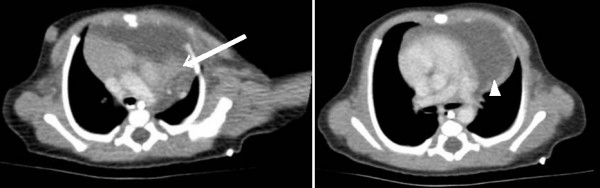
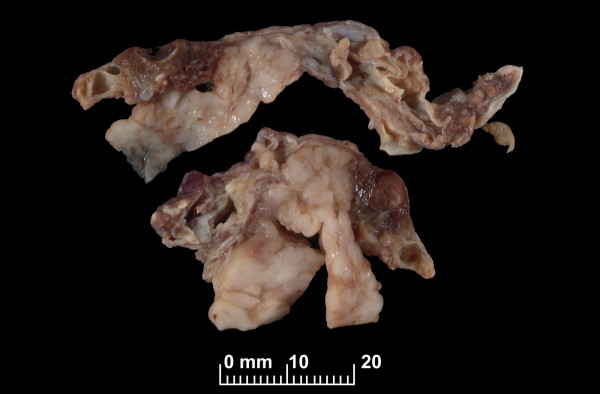
Case presentation: We report one such case that was mistaken for other entities in both the prenatal and immediate post-natal period. Initial and follow-up antenatal ultrasound scans demonstrated a multicystic lesion in the left chest, and the mother was counselled about the possibility of her baby having a congenital diaphragmatic hernia. Initial post-natal chest radiographs were reported as normal. An echocardiogram and thoracic computed tomography scan confirmed a complex multiloculated cystic mediastinal mass. The working diagnoses were of a mediastinal teratoma or congenital cystic adenomatous malformation. At operation, the lesion was compressed by the left lung and was found to be close to the left phrenic nerve, which was carefully identified and preserved. After excision, histopathological examination of the mass confirmed the diagnosis of cystic hygroma. Postoperative dyspnoea was observed secondary to paradoxical movement of the left hemidiaphragm and probable left phrenic neuropraxia. This settled conservatively with excellent recovery.
Conclusion: Despite the fact that isolated intrathoracic cystic hygroma is a rare entity, it needs to be considered in the differential diagnosis of foetal and neonatal mediastinal masses, particularly for juxtadiaphragmatic lesions. The phrenic nerve is not identifiable on prenatal ultrasound imaging, and it is therefore understandable that a mass close to the diaphragm may be mistaken for a congenital diaphragmatic hernia because of the location, morphology and potential phrenic nerve compression. Post-natal diagnosis may also be misleading as many mediastinal cystic masses have similar appearances on imaging. Therefore, as well as cystic architecture, special consideration needs to be given to the anatomical location and effect on local structures.
Figures
References
-
- Omell GH, Anderson LS, Bramson RT. Chest wall tumors. Radiol Clin North Am. 1973;11:197–214. - PubMed
-
- Redenbacker EAH. De Ranula Sublingua, Speciali, cum Casa Congenita. Monachii, Lindhaue. 1828.
-
- Glasson MJ, Taylor SF. Cervical, cervicomediastinal and intrathoracic lymphangioma. Prog Pediatr Surg. 1991;27:62–83. - PubMed
LinkOut - more resources
Full Text Sources
