

Current concepts in management of oral cancer--surgery
- PMID: 18674952
- PMCID: PMC4130348
- DOI: 10.1016/j.oraloncology.2008.05.017
Current concepts in management of oral cancer--surgery
Abstract
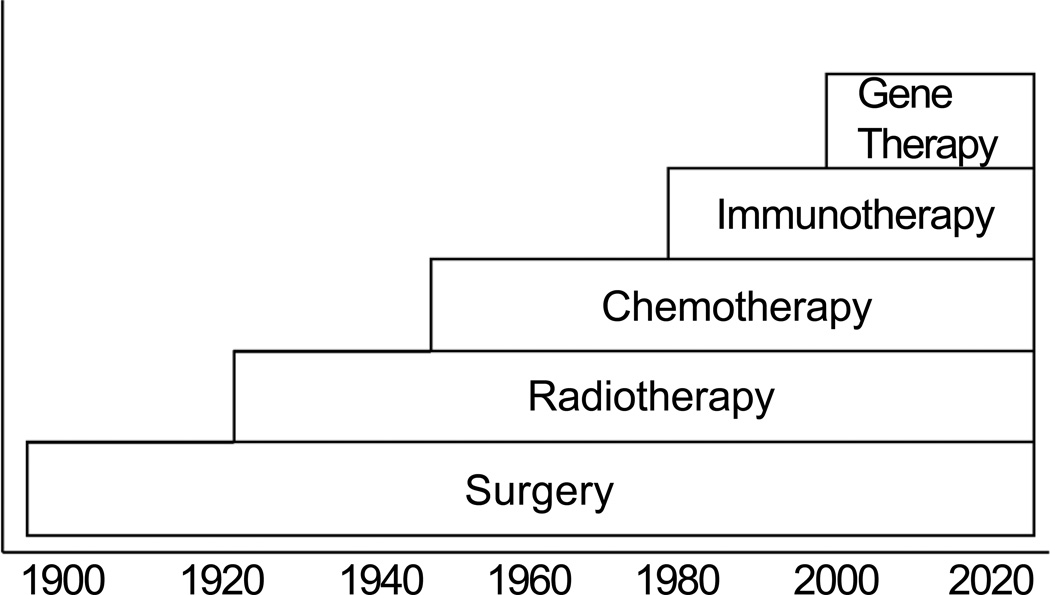
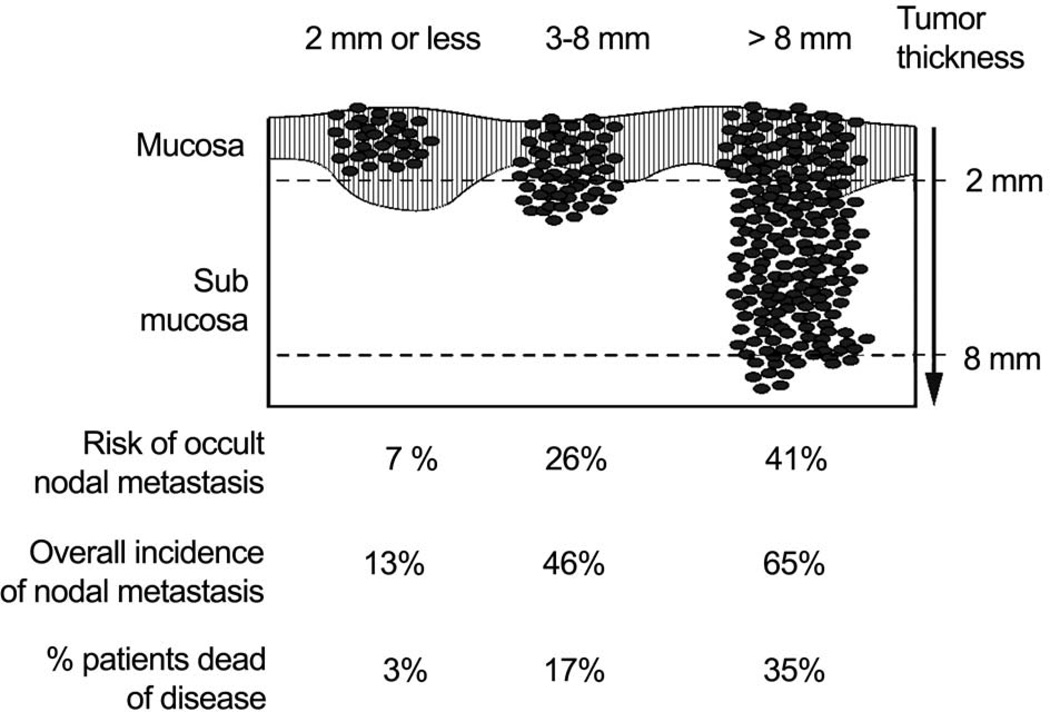
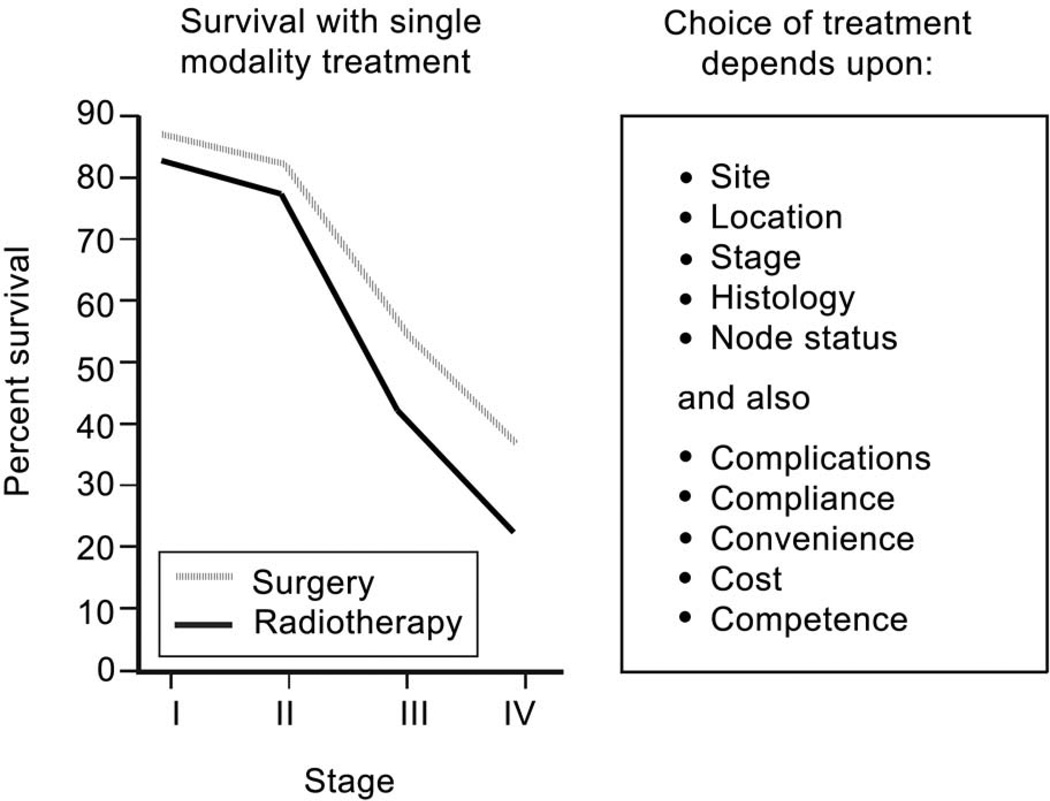
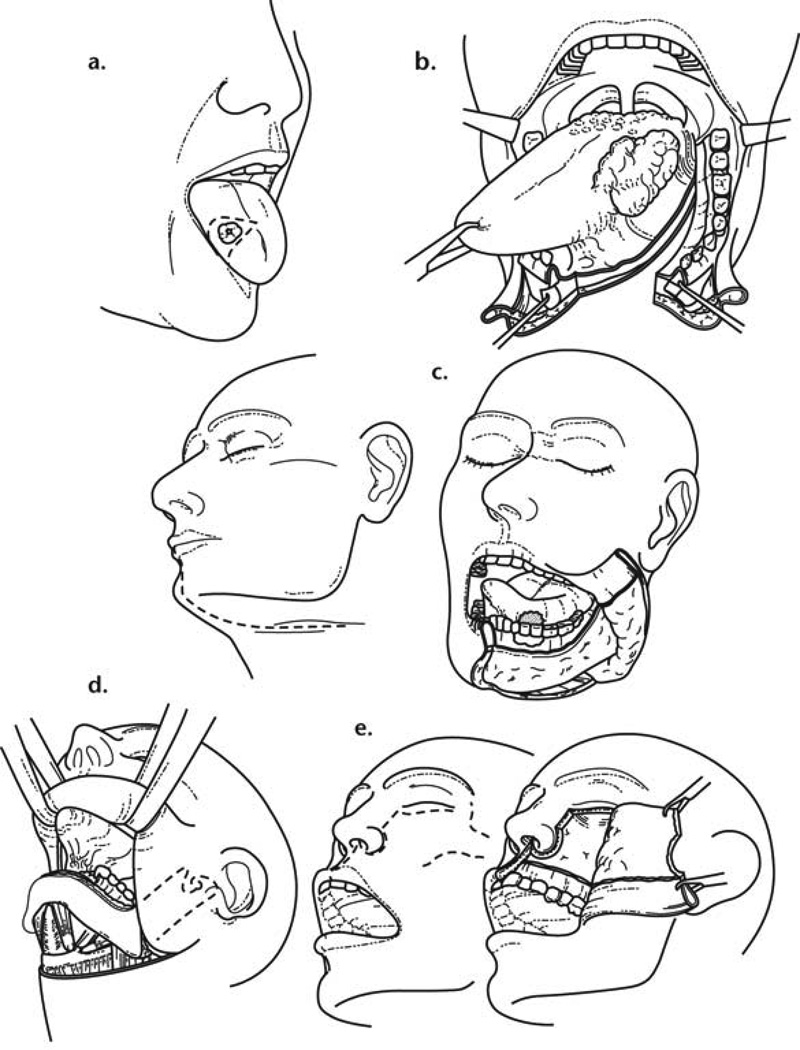
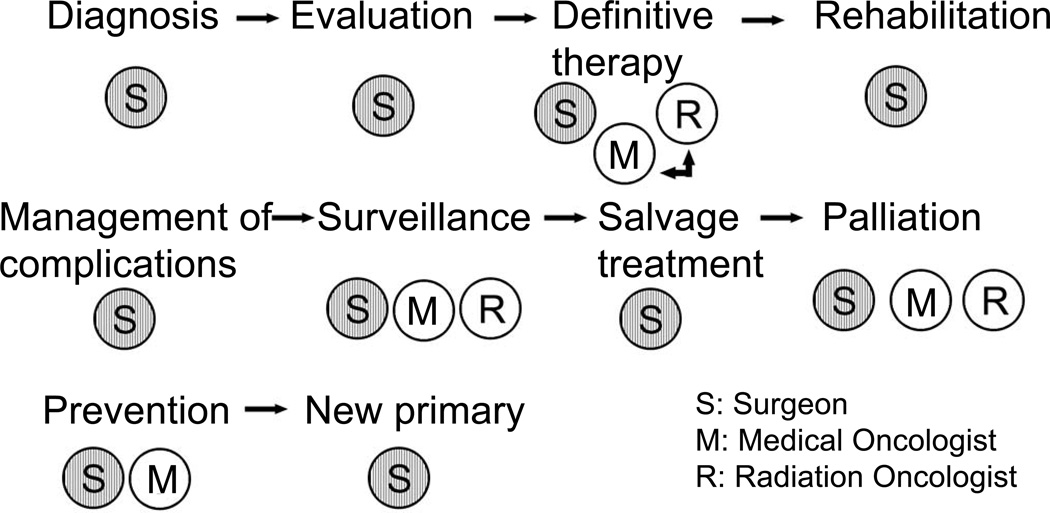
Oral cancer is the sixth most common cancer worldwide, with a high prevalence in South Asia. Tobacco and alcohol consumption remain the most dominant etiologic factors, however HPV has been recently implicated in oral cancer. Surgery is the most well established mode of initial definitive treatment for a majority of oral cancers. The factors that affect choice of treatment are related to the tumor and the patient. Primary site, location, size, proximity to bone, and depth of infiltration are factors which influence a particular surgical approach. Tumors that approach or involve the mandible require specific understanding of the mechanism of bone involvement. This facilitates the employment of mandible sparing approaches such as marginal mandibulectomy and mandibulotomy. Reconstruction of major surgical defects in the oral cavity requires use of a free flap. The radial forearm free flap provides excellent soft tissue and lining for soft tissue defects in the oral cavity. The fibula free flap remains the choice for mandibular reconstruction. Over the course of the past thirty years there has been improvement in the overall survival of patients with oral carcinoma largely due to the improved understanding of the biology of local progression, early identification and treatment of metastatic lymph nodes in the neck, and employment of adjuvant post-operative radiotherapy or chemoradiotherapy. The role of surgery in primary squamous cell carcinomas in other sites in the head and neck has evolved with integration of multidisciplinary treatment approaches employing chemotherapy and radiotherapy either sequentially or concurrently. Thus, larynx preservation with concurrent chemoradiotherapy has become the standard of care for locally advanced carcinomas of the larynx or pharynx requiring total laryngectomy. On the other hand, for early staged tumors of the larynx and pharynx, transoral laser microsurgery has become an effective means of local control of these lesions. Advances in skull base surgery have significantly improved the survivorship of patients with malignant tumors of the paranasal sinuses approaching or involving the skull base. Surgery thus remains the mainstay of management of a majority of neoplasms arising in the head and neck area. Similarly, the role of the surgeon is essential throughout the life history of a patient with a malignant neoplasm in the head and neck area, from initial diagnosis through definitive treatment, post-treatment surveillance, management of complications, rehabilitation of the sequelae of treatment, and finally for palliation of symptoms.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
None declared.
Figures
References
-
- Moore SR, Johnson NW, Pierce AM, Wilson DF. The epidemiology of mouth cancer: a review of global incidence. Oral Dis. 2000;6:65–74. - PubMed
-
- Sankaranarayanan R. Oral cancer in India: a clinical and epidemiological review. Oral Surg Oral Med Oral Pathol. 1990;69:325–330. - PubMed
-
- Endicott N, Jensen R, Lyman G, et al. Adjuvant chemotherapy for advanced head and neck squamous carcinoma. Cancer. 1987 Jun;60:301–311. - PubMed
-
- Shah JP, Patel SG. Head and Neck Surgery and Oncology. 3rd Edition. Edinburgh, London, New York: Mosby; 2003.
-
- Shah JP. Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg. 1990 Oct;160(4):405–409. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
