

Determinants of lung volumes in chronic spinal cord injury
- PMID: 18674986
- PMCID: PMC2647858
- DOI: 10.1016/j.apmr.2008.02.018
Determinants of lung volumes in chronic spinal cord injury
Abstract
Objective: To characterize determinants of lung volumes in chronic spinal cord injury (SCI).
Design: Cross-sectional.
Setting: VA Boston Healthcare System.
Participants: White men (N=330) with chronic SCI.
Interventions: Not applicable.
Main outcome measures: Questionnaire responses and measurements of lung volumes.
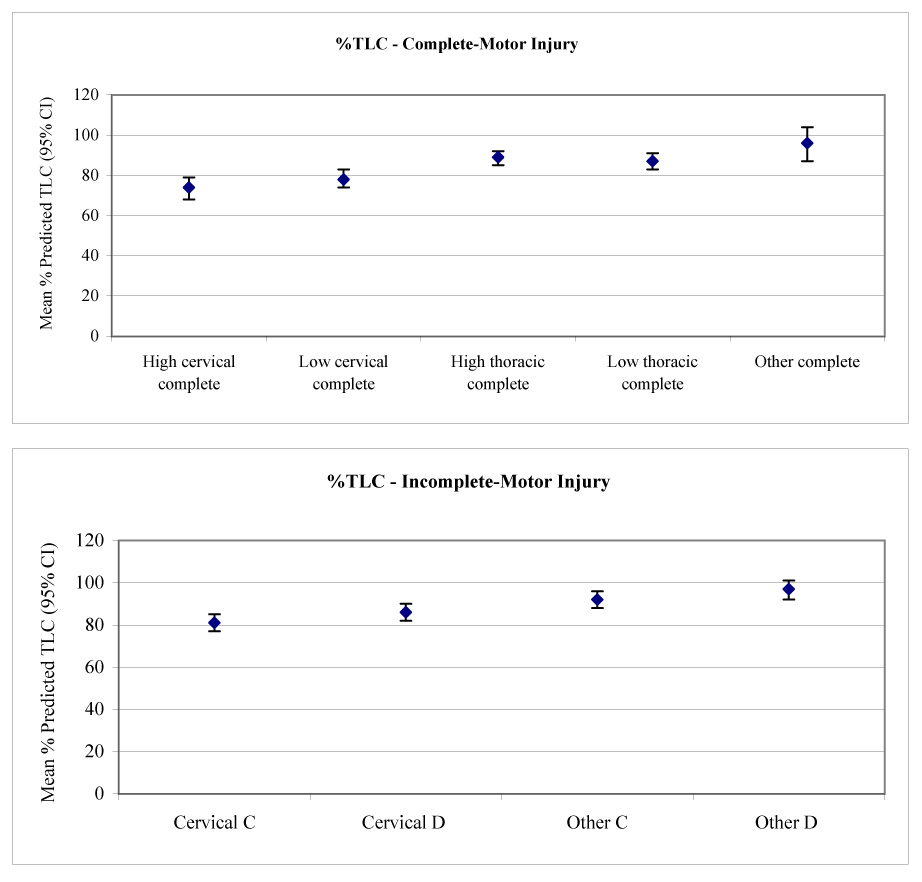
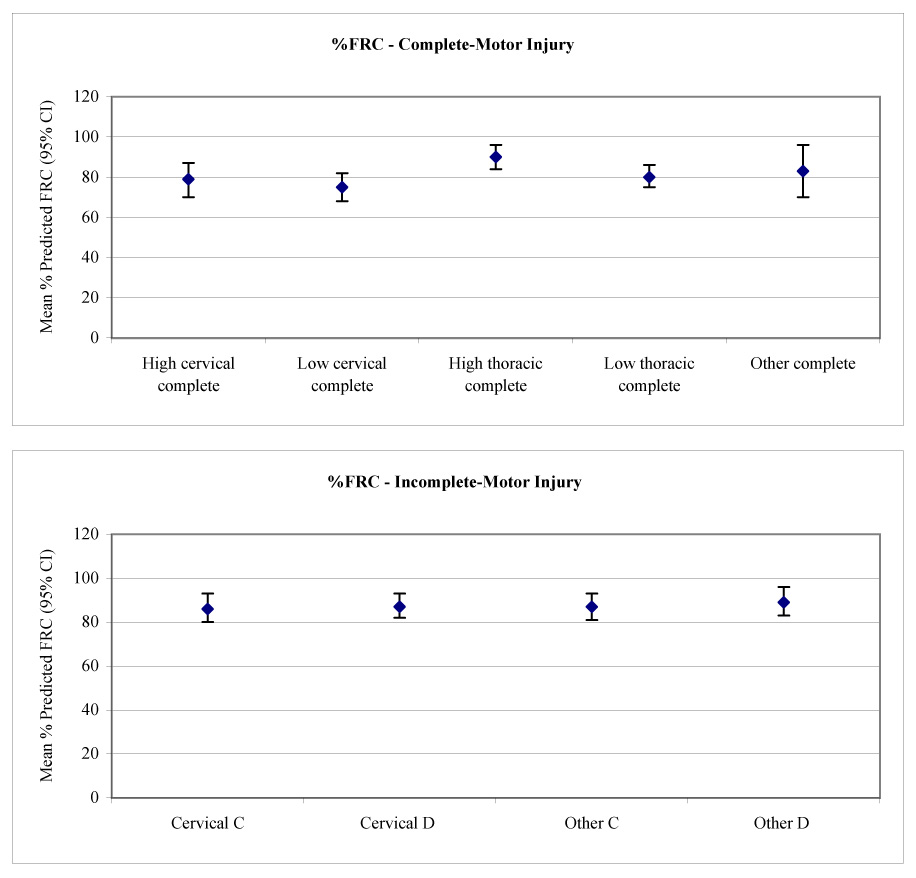
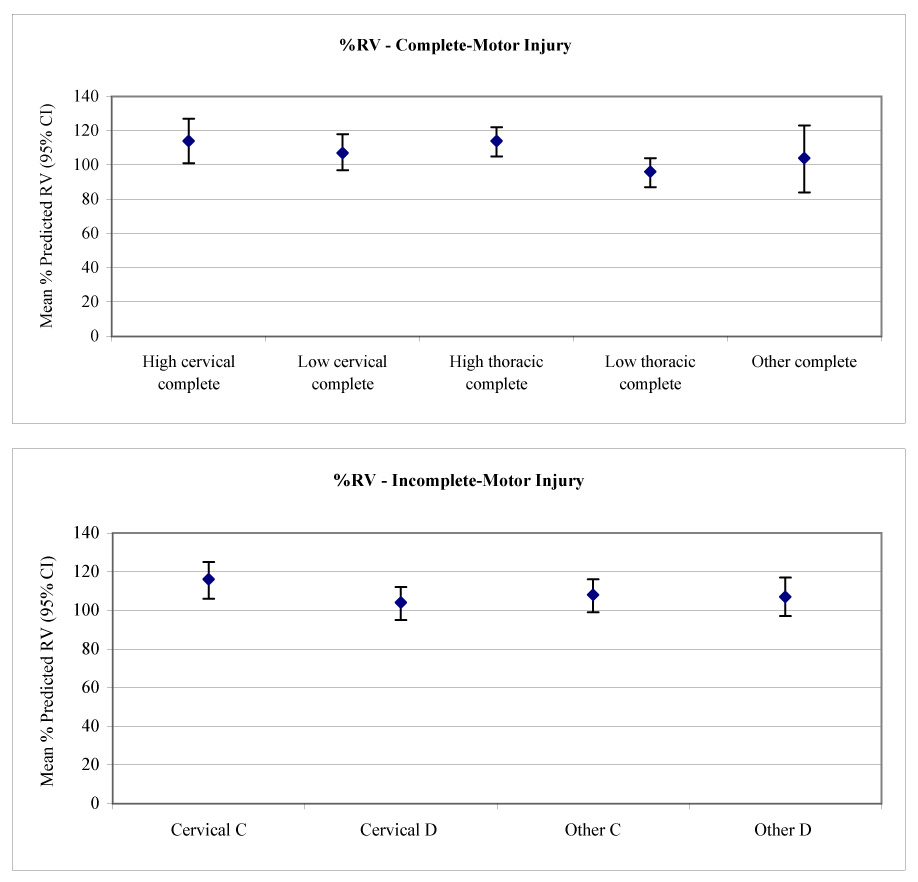
Results: Adjusted for SCI severity and stature, greater body mass index (BMI) was associated (all P<.05) with lower total lung capacity (TLC) (-38.7 mL x kg(-1) x m(-2)), functional residual capacity (FRC) (-73.9 mL x kg(-1) x m(-2)), residual volume (RV) (-40.4 mL x kg(-1) x m(-2)), and expiratory reserve volume (ERV) (-32.2 mL x kg(-1) x m(-2)). The effect of BMI on RV was most pronounced in quadriplegia (-72 mL x kg(-1) x m(-2)). Lifetime smoking was associated with a greater FRC (5.3 mL/pack-year) and RV (3.1 mL/pack-years). The effects of lifetime smoking were also greatest in quadriplegia (11 mL/pack-year for FRC; 7.8 mL/pack-year for RV). Time since injury, independent of age, was associated with a decrease in TLC, FRC, ERV, and RV (P<.05). Age was not a predictor of TLC once time since injury was considered.
Conclusions: Determinants of FRC, TLC, ERV, and RV in chronic SCI include factors related and unrelated to SCI. The mechanisms remain to be determined but likely involve the elastic properties and muscle function of the respiratory system and perhaps the effects of systemic inflammation related to adiposity. Addressing modifiable factors such as obesity, muscle stiffness, and smoking may improve respiratory morbidity and mortality in SCI by improving pulmonary function.
Figures
References
-
- DeVivo MJ, Stover SL. Long term survival and causes of death. In: Stover SL, DeLisa JA, Whiteneck GG, editors. Spinal cord injury clinical outcomes from the model systems. Gaithersburg: Aspen; 1995. pp. 289–316.
-
- DeVivo MJ, Black KJ, Stover SL. Causes of death during the first 12 years after spinal cord injury. Arch Phys Med Rehabil. 1993;74:248–254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
