

Efficacy of site-independent telemedicine in the STRokE DOC trial: a randomised, blinded, prospective study
- PMID: 18676180
- PMCID: PMC2744128
- DOI: 10.1016/S1474-4422(08)70171-6
Efficacy of site-independent telemedicine in the STRokE DOC trial: a randomised, blinded, prospective study
Abstract
Background: To increase the effective use of thrombolytics for acute stroke, the expertise of vascular neurologists must be disseminated more widely. We prospectively assessed whether telemedicine (real-time, two-way audio and video, and digital imaging and communications in medicine [DICOM] interpretation) or telephone was superior for decision making in acute telemedicine consultations.
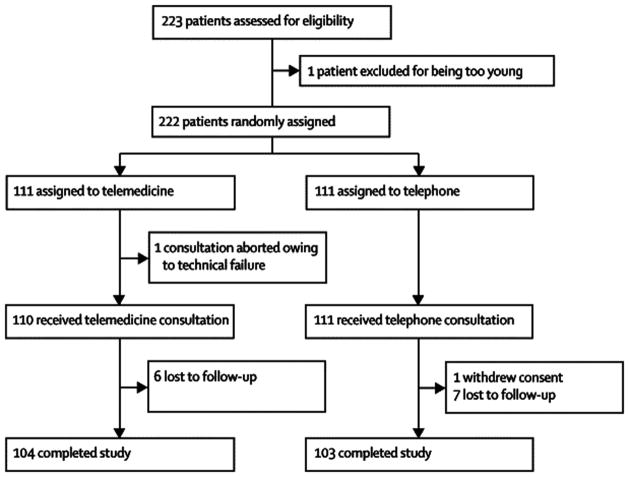
Methods: From January, 2004, to August, 2007, patients older than 18 years who presented with acute stroke symptoms at one of four remote spoke sites were randomly assigned, through a web-based, permuted blocks system, to telemedicine or telephone consultation to assess their suitability for treatment with thrombolytics, on the basis of standard criteria. The primary outcome measure was whether the decision to give thrombolytic treatment was correct, as determined by central adjudication. Secondary outcomes were the rate of thrombolytic use, 90-day functional outcomes (Barthel index [BI] and modified Rankin scale [mRS]), the incidence of intracerebral haemorrhages, and technical observations. Analysis was by intention to treat. This trial is registered with ClinicalTrials.gov, number NCT00283868.
Findings: 234 patients were assessed prospectively. 111 patients were randomised to telemedicine, and 111 patients were randomised to telephone consultation; 207 completed the study. Mean National Institutes of Health stroke scale score at presentation was 9.5 (SD 8.1) points (11.4 [8.7] points in the telemedicine group versus 7.7 [7.0] points in the telephone group; p=0.002). One telemedicine consultation was aborted for technical reasons, although it was included in the analyses. Correct treatment decisions were made more often in the telemedicine group than in the telephone group (108 [98%] vs 91 [82%], odds ratio [OR] 10.9, 95% CI 2.7-44.6; p=0.0009). Intravenous thrombolytics were used at an overall rate of 25% (31 [28%] telemedicine vs 25 [23%] telephone, 1.3, 0.7-2.5; p=0.43). 90-day functional outcomes were not different for BI (95-100) (0.6, 0.4-1.1; p=0.13) or for mRS score (0.6, 0.3-1.1; p=0.09). There was no difference in mortality (1.6, 0.8-3.4; p=0.27) or rates of intracerebral haemorrhage after treatment with thrombolytics (2 [7%] telemedicine vs 2 [8%] telephone, 0.8, 0.1-6.3; p=1.0). However, there were more incomplete data in the telephone group than in the telemedicine group (12%vs 3%, 0.2, 0.1-0.3; p=0.0001).
Interpretation: The authors of this trial report that stroke telemedicine consultations result in more accurate decision making compared with telephone consultations and can serve as a model for the effectiveness of telemedicine in other medical specialties. The more appropriate decisions, high rates of thrombolysis use, improved data collection, low rate of intracerebral haemorrhage, low technical complications, and favourable time requirements all support the efficacy of telemedicine for making treatment decisions, and might enable more practitioners to use this medium in daily stroke care.
Conflict of interest statement
Dr. Meyer had full access to all of the data in the study and had final responsibility for the decision to submit for publication. There are no conflicts of interest to disclose.
Comment in
-
"Telethrombolysis": stroke consultation by telemedicine.Lancet Neurol. 2008 Sep;7(9):763-5. doi: 10.1016/S1474-4422(08)70172-8. Lancet Neurol. 2008. PMID: 18676181 No abstract available.
References
-
- Reeves MJ, Arora S, Broderick JP, et al. Acute stroke care in the US: results from 4 pilot prototypes of the Paul Coverdell National Acute Stroke Registry. Stroke. 2005;36:1232–1240. - PubMed
-
- Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:768–774. - PubMed
-
- The NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Katzan IL, Furlan AJ, Lloyd LE, et al. Use of Tissue-Type Plasminogen Activator for Acute Ischemic Stroke: The Cleveland Area Experience. Journal of the American Medical Association. 2000;283:1151–1158. - PubMed
-
- Sable CA, Cummings SD, Pearson GD, et al. Impact of Telemedicine on the Practice of Pediatric Cardiology in Community Hospitals. Pediatrics. 2002;109:1–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
